Downloaded 348 times





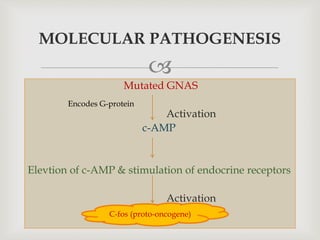



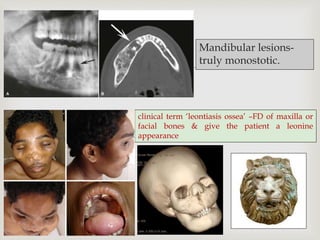











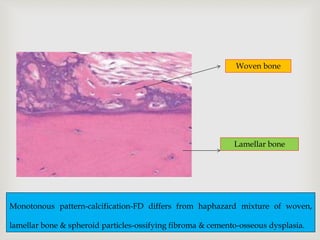






This document provides an overview of fibro-osseous lesions and focuses on fibrous dysplasia. It discusses the classification, etiology, clinical features, radiographic features, histologic features, treatment and prognosis of fibrous dysplasia. Fibrous dysplasia is a benign bone lesion caused by a mutation in the GNAS1 gene. It can present as monostotic, polyostotic or craniofacial lesions. Radiographically, it appears as radiolucent or radiopaque areas with a "ground glass" appearance. Histologically, it is characterized by fibrous tissue and irregular woven bone trabeculae. Treatment involves surgery or bisphosphonates and the prognosis is generally good

















































































