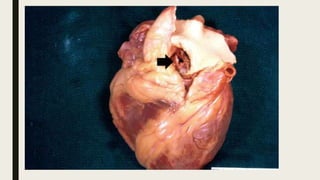
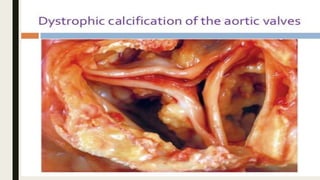
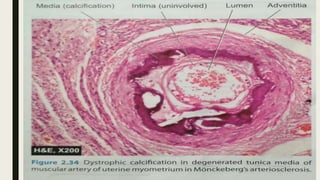
Pathological calcification involves the abnormal deposition of calcium salts in tissues other than bone. There are two main types: dystrophic calcification occurs in dead or damaged tissue with normal calcium levels, while metastatic calcification affects normal tissues and results from disorders that increase calcium levels in the blood (hypercalcemia). Dystrophic calcification is seen in areas of necrosis, atherosclerotic plaques, and infarcts. Metastatic calcification commonly involves the kidneys, lungs, blood vessels, and stomach, and is caused by hyperparathyroidism, bone destruction, or excessive vitamin D intake.