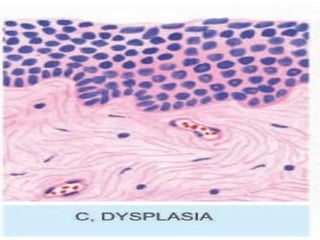
The document discusses cellular adaptations necessary for survival under stress, highlighting various mechanisms such as atrophy, hypertrophy, hyperplasia, metaplasia, and dysplasia. It outlines physiological and pathological causes for these adaptations, detailing outcomes that can range from reversible changes to potential cancer development. The concept 'survival of the adaptable' illustrates the importance of these cellular responses in maintaining homeostasis or leading to disease if stimuli persist.