This document discusses the investigation and management of atrial septal defects (ASD). Key points include:
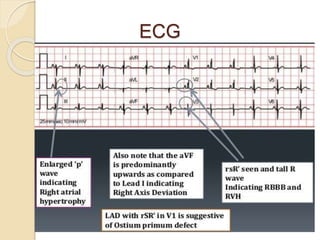
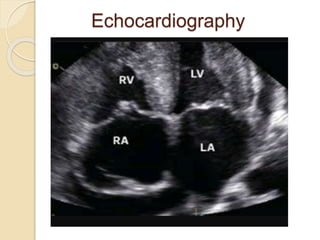
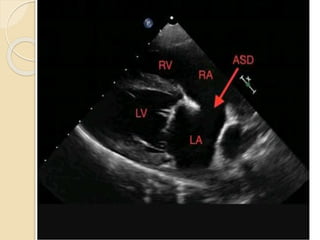
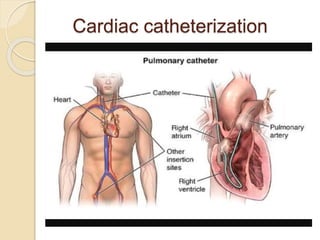
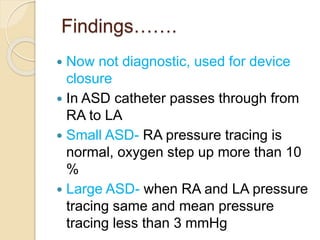
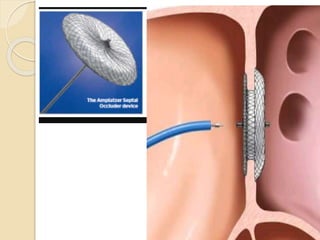
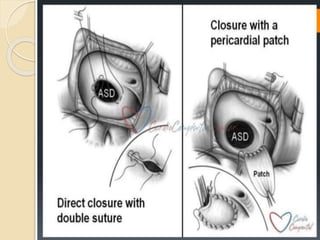
ECG, echocardiography, chest x-ray and cardiac catheterization are used to diagnose ASD. Echocardiography can image the interatrial septum from various views and detect flow between the atria with color Doppler. ASDs are often asymptomatic but can cause complications like pulmonary hypertension. Small and moderate ASDs may be treated with percutaneous device closure while larger defects or those with complications may require surgical repair via patch. The take home message is that small ASDs can often be asymptomatic for life while larger defects cause issues in adulthood, and definitive treatment is via device








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















