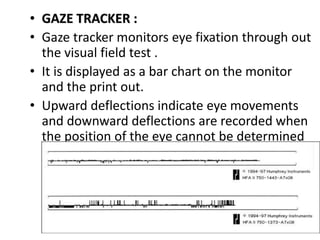
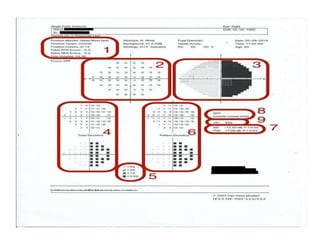
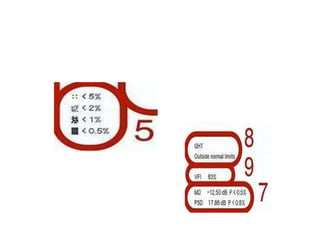
The document defines the visual field and describes methods for examining it, including confrontation testing, tangent screen testing, Amsler grid testing, static and kinetic perimetry, and Humphrey Field Analyzer (HFA) testing. It discusses the normal limits of the visual field and reliability indices used to evaluate HFA test results, such as fixation losses, false positives, and false negatives. Single field analysis results from the HFA including sensitivity values, gray scale maps, and total and pattern deviation plots are also summarized.