Download as PDF, PPTX








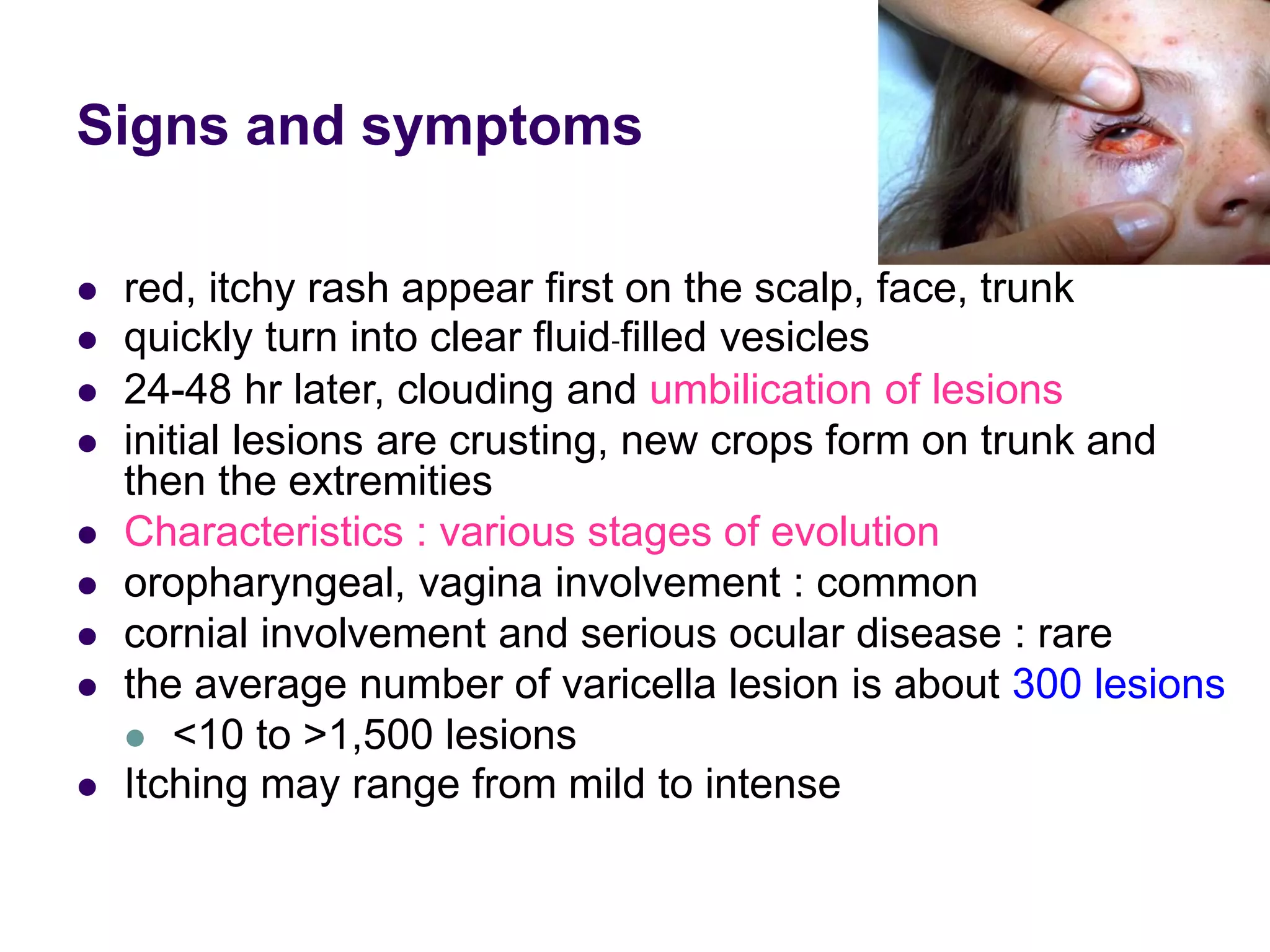













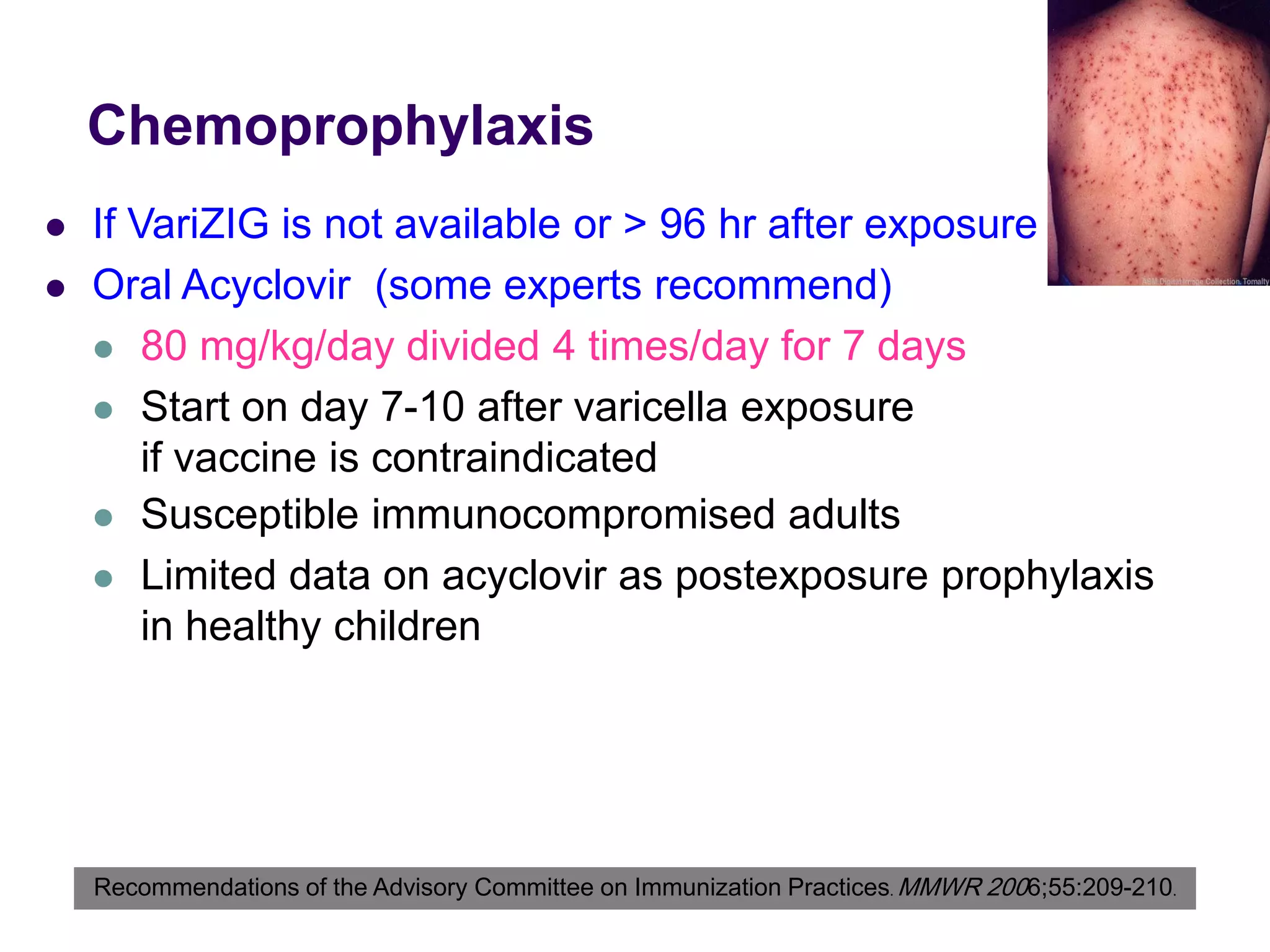
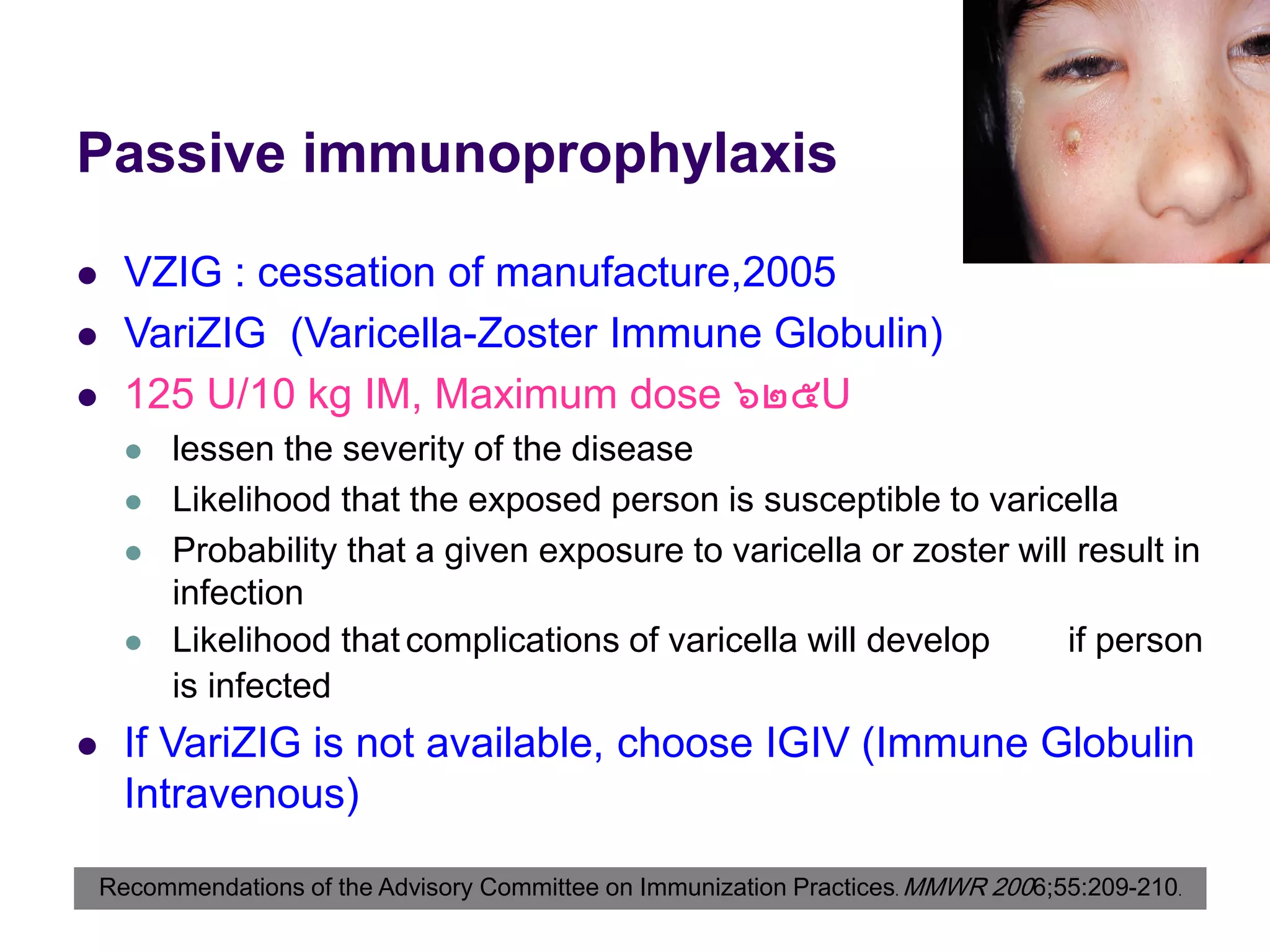
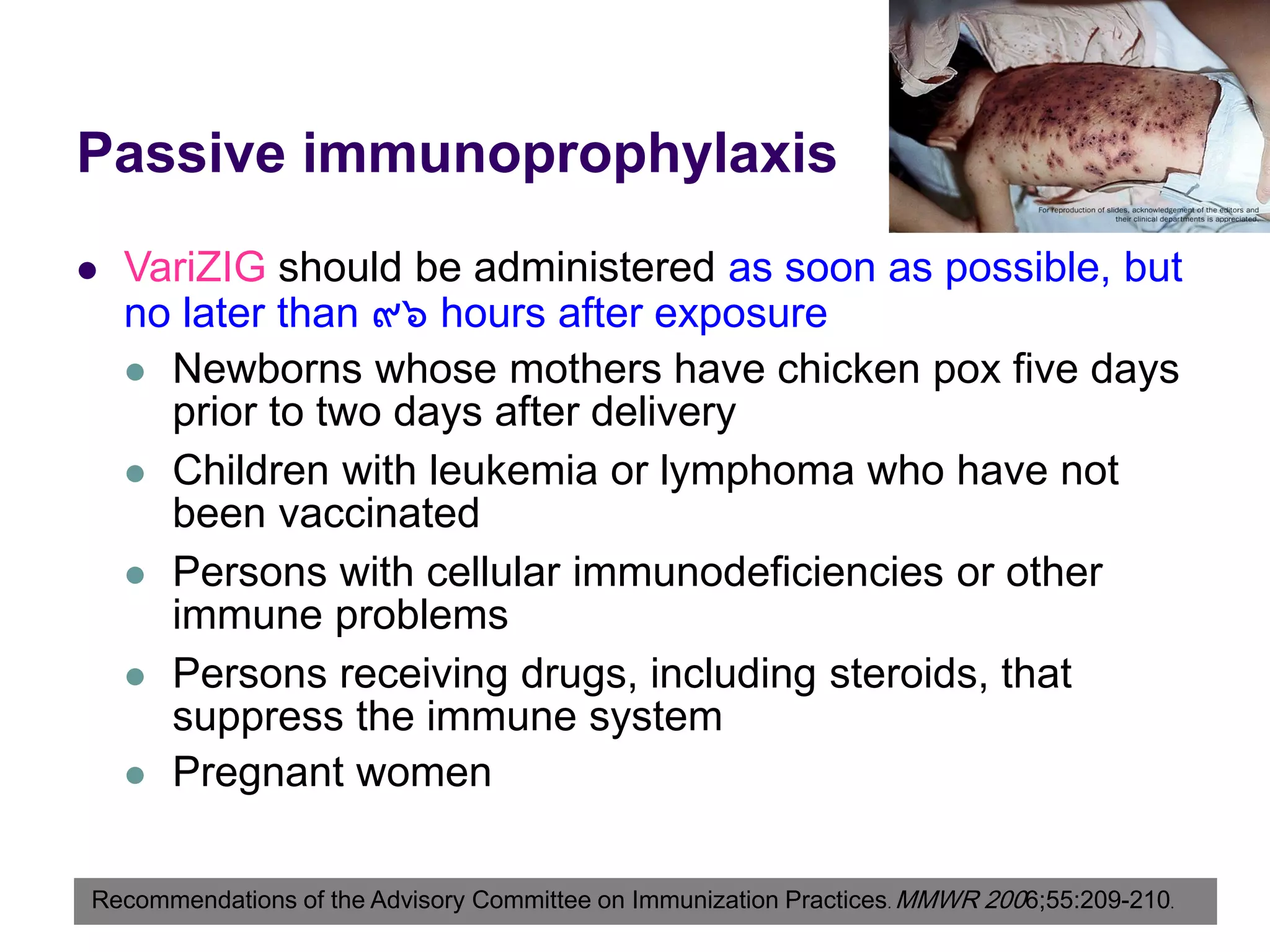








































This document discusses Varicella-Zoster Virus, which causes chickenpox and shingles. It describes how chickenpox is highly contagious and mainly affects children, while shingles results from reactivation of the virus in nerve ganglia and mainly affects adults and immunocompromised individuals. Complications can be more severe in adults, newborns and immunocompromised patients. Treatment involves antiviral medications like acyclovir to reduce symptoms and duration. Vaccination and immune globulin can help prevent or lessen the disease in high-risk groups following exposure.











































































































