Downloaded 513 times

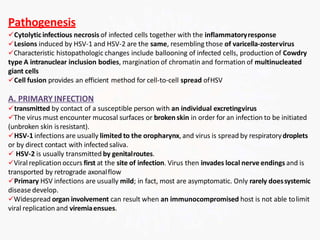
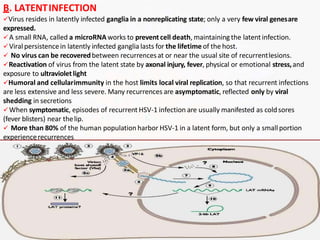
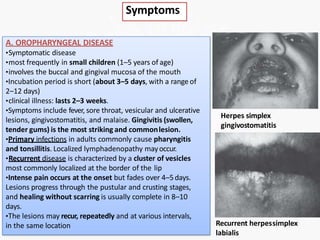
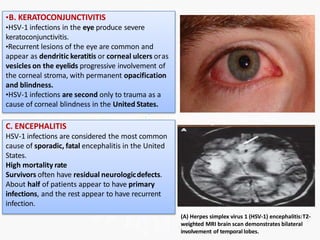
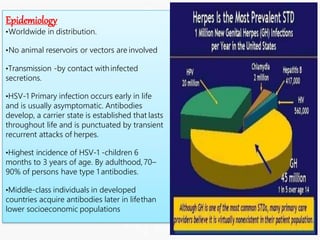







The document discusses human herpesvirus infections, focusing on herpes simplex viruses types 1 and 2. It provides details on the structure and properties of herpesviruses, describing how they cause both lytic and latent infections. The major symptoms and clinical manifestations of HSV-1 and HSV-2 infections are outlined, including oral and genital lesions as well as infections in immunocompromised individuals and newborns. Recurrent infections are also discussed.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










