
Downloaded 229 times















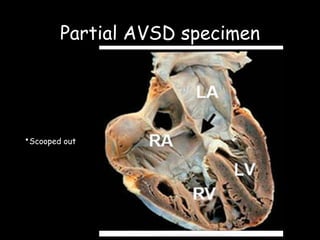
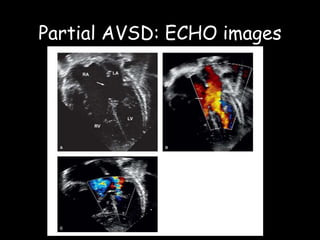
















































This document discusses atrioventricular septal defects (AVSDs), including their embryogenesis, classification, clinical features, imaging, and management. It describes the spectrum of AVSDs from partial to complete. Partial AVSDs involve a primum atrial septal defect with a cleft in the mitral valve. Complete AVSDs have a large ventricular septal defect with a common atrioventricular valve. Imaging like echocardiography is important for evaluating the anatomy and determining appropriate treatment, which ranges from observation to surgical repair.























































































