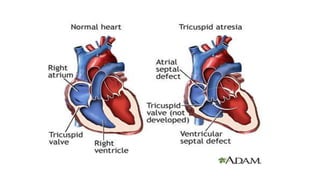
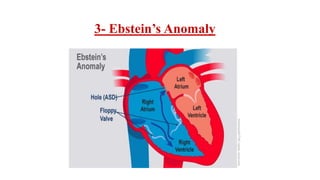
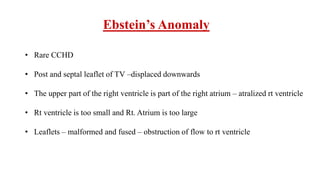
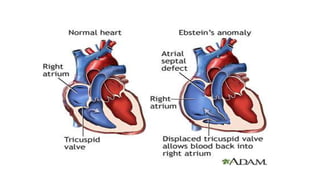
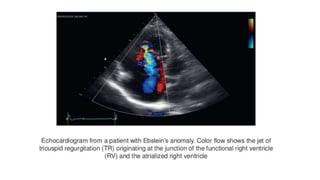
1. Ebstein's anomaly is a rare congenital heart defect where the tricuspid valve is displaced downward into the right ventricle, causing obstruction of blood flow.
2. This leads to a shunt of deoxygenated blood from the right to left atrium, causing cyanosis.
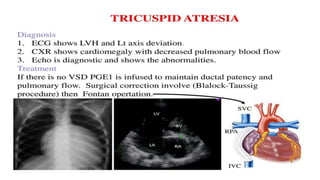
3. Surgical options include tricuspid valve repair or replacement, closure of intra-atrial communications, and reduction of the enlarged right atrium and right ventricle. The goal is to improve valve function and cardiac output while eliminating arrhythmias.


























































![cyanotic congenital heart disease[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cyanoticcongenitalheartdisease1-250421184527-f500caa9-thumbnail.jpg?width=640&height=640&fit=bounds)



















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








