Downloaded 254 times



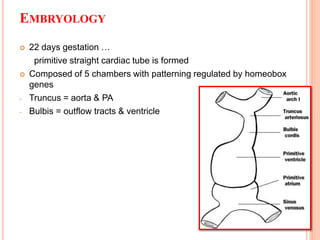




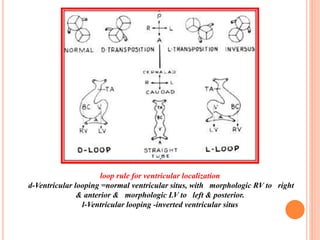


































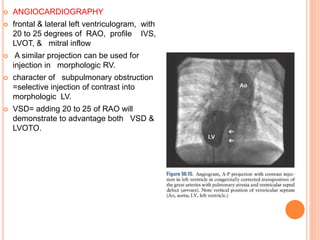


























This document discusses the anatomy, embryology, and management of L-TGA (transposition of the great arteries). Some key points: - In L-TGA, the ventricles are inverted such that the morphologic right ventricle is on the left and pumps blood to the lungs, while the morphologic left ventricle is on the right and pumps blood to the body. - Embryologically, abnormal leftward looping of the heart tube during development results in the inverted ventricles. The conduction system and coronary arteries also have abnormal anatomy. - Clinical features may include congenital heart block, progressive tricuspid regurgitation, pulmonary stenosis, and heart failure. Diagn























































































