
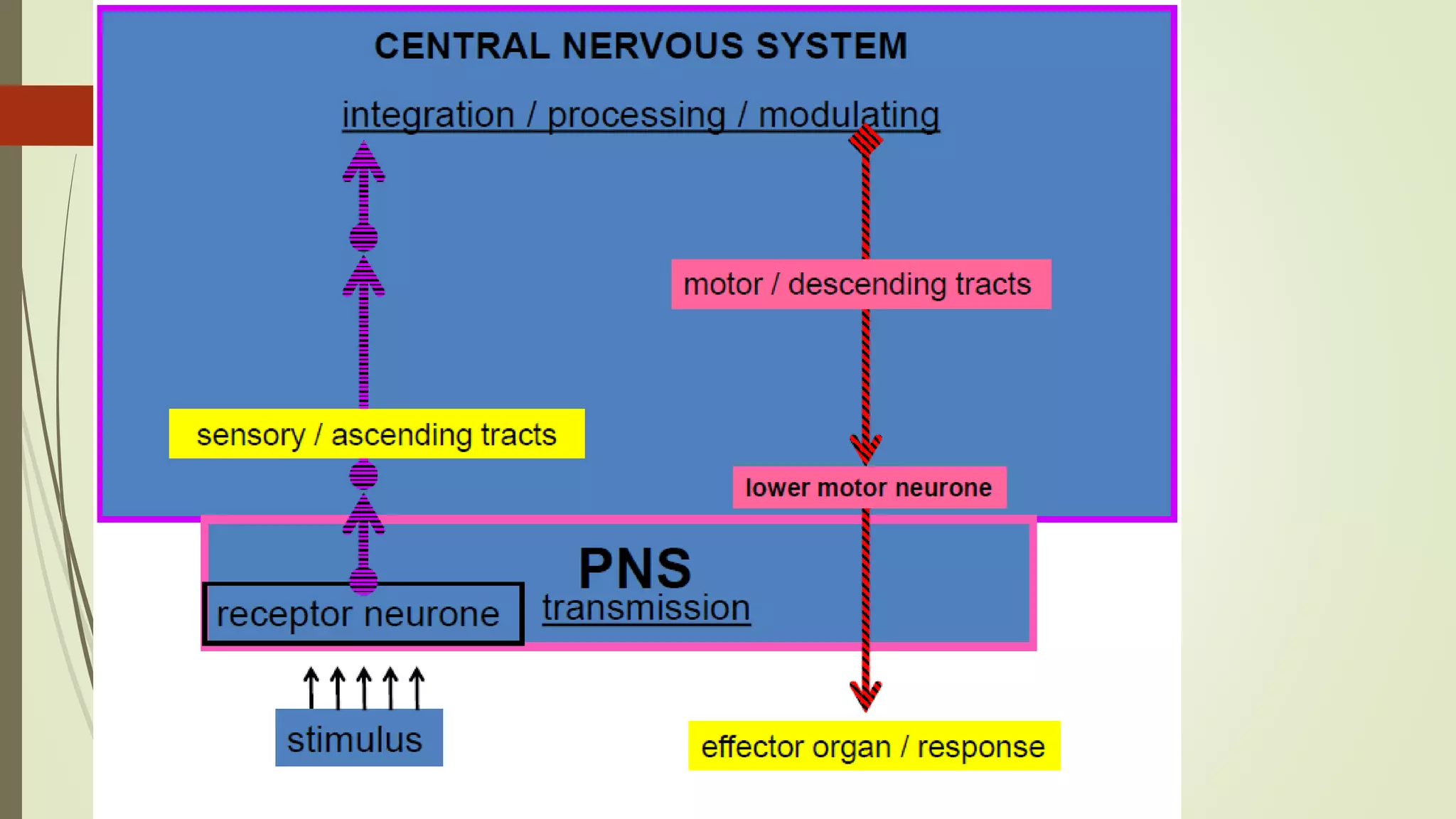
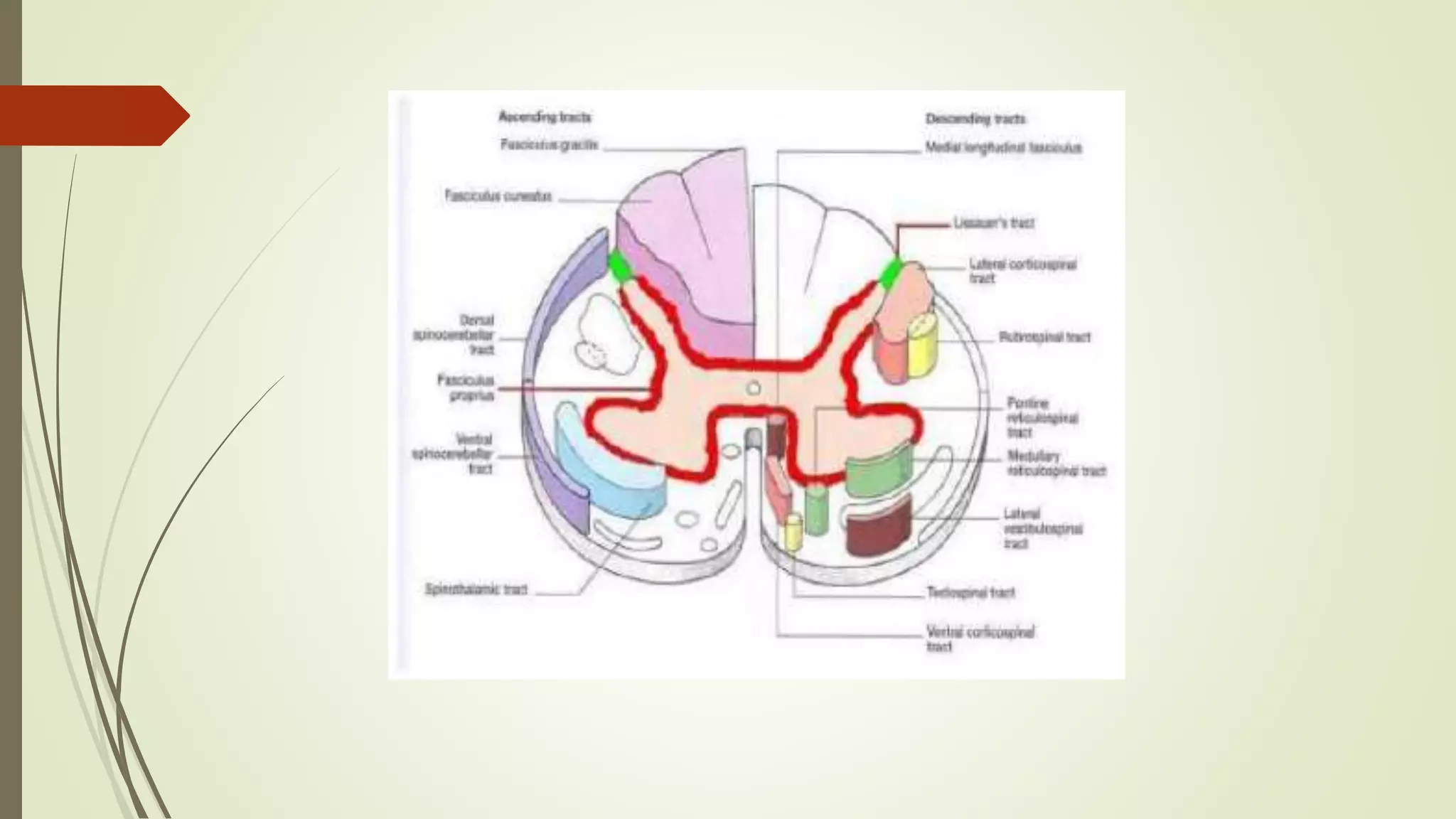
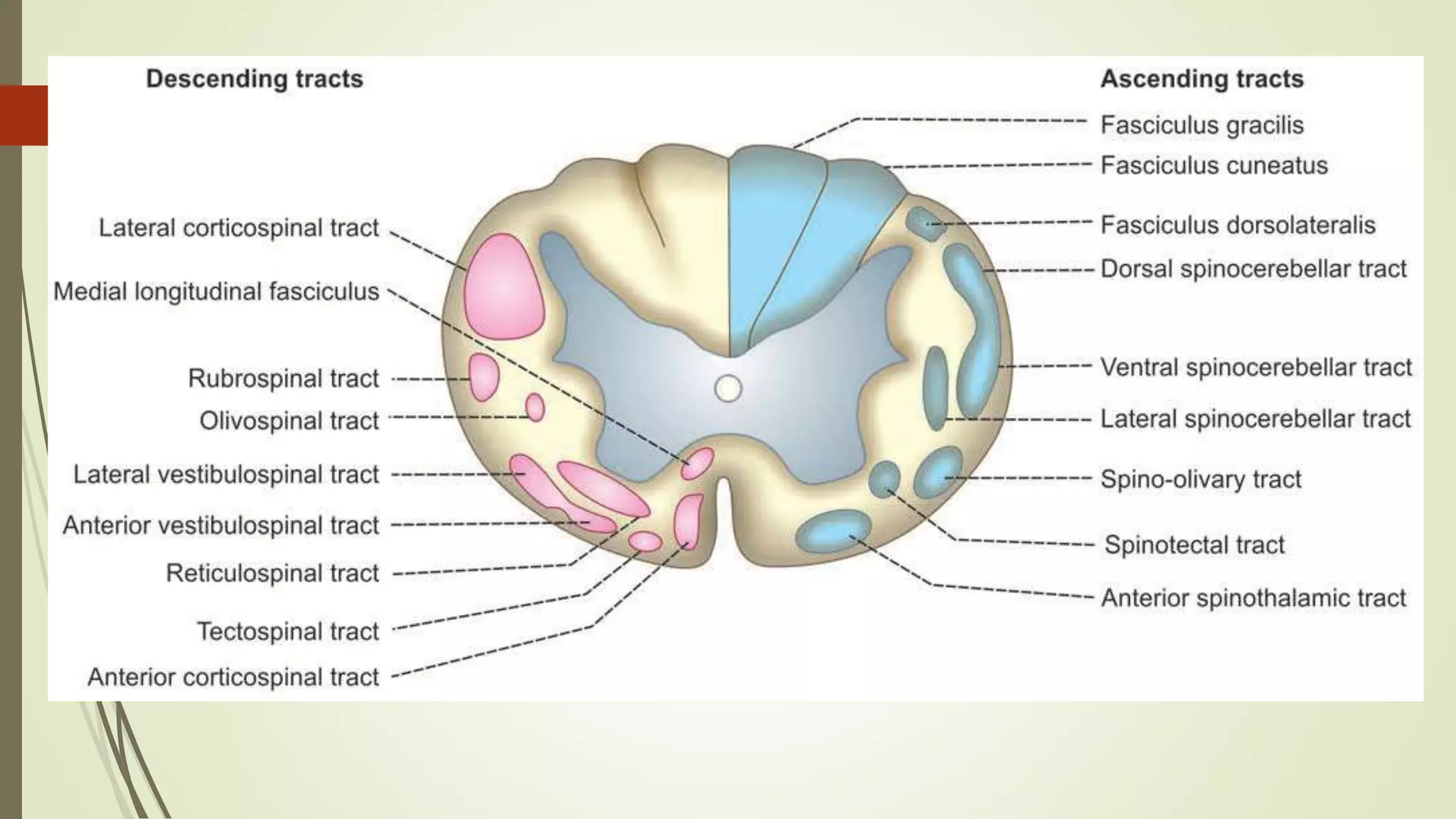
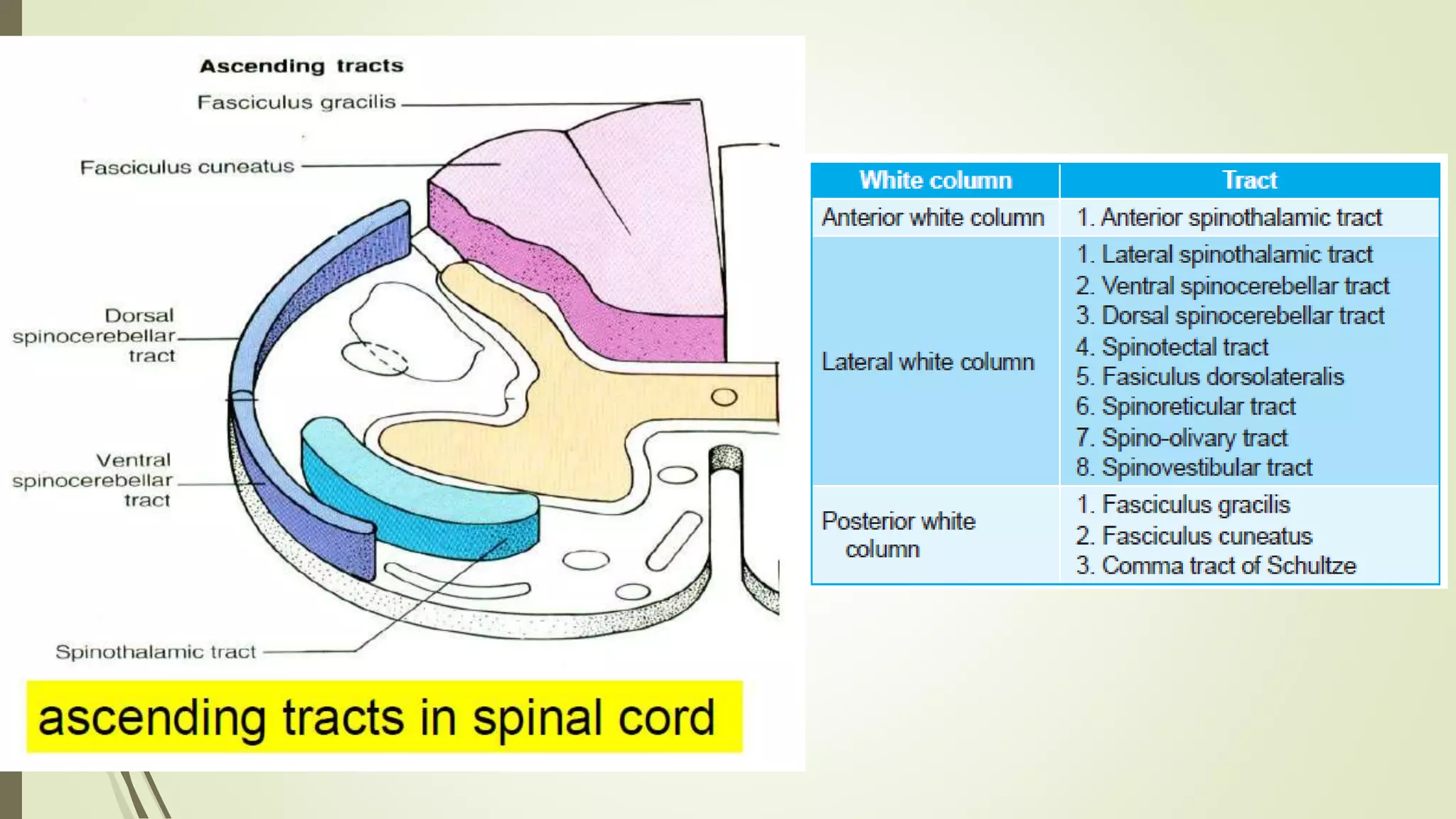

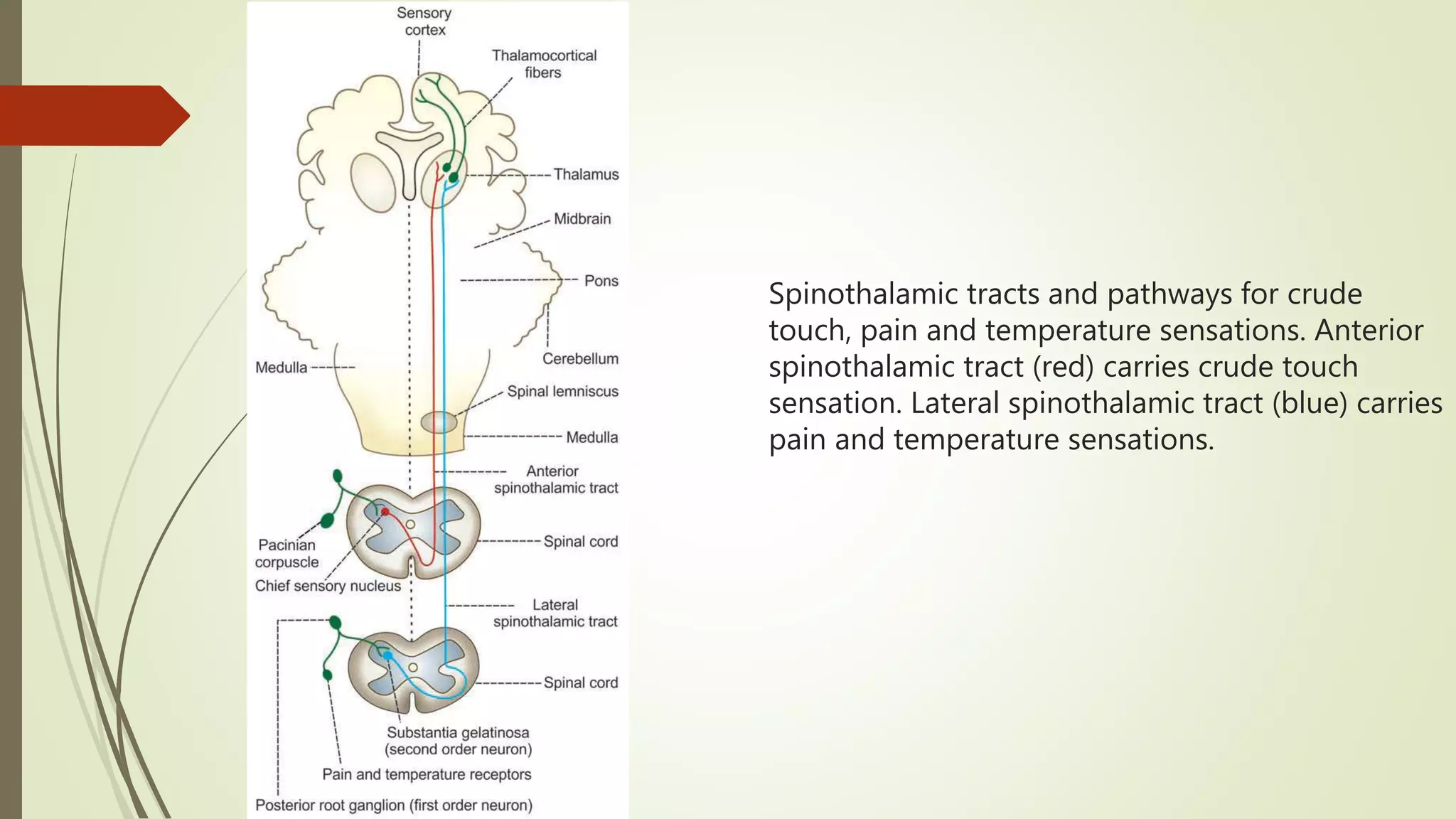
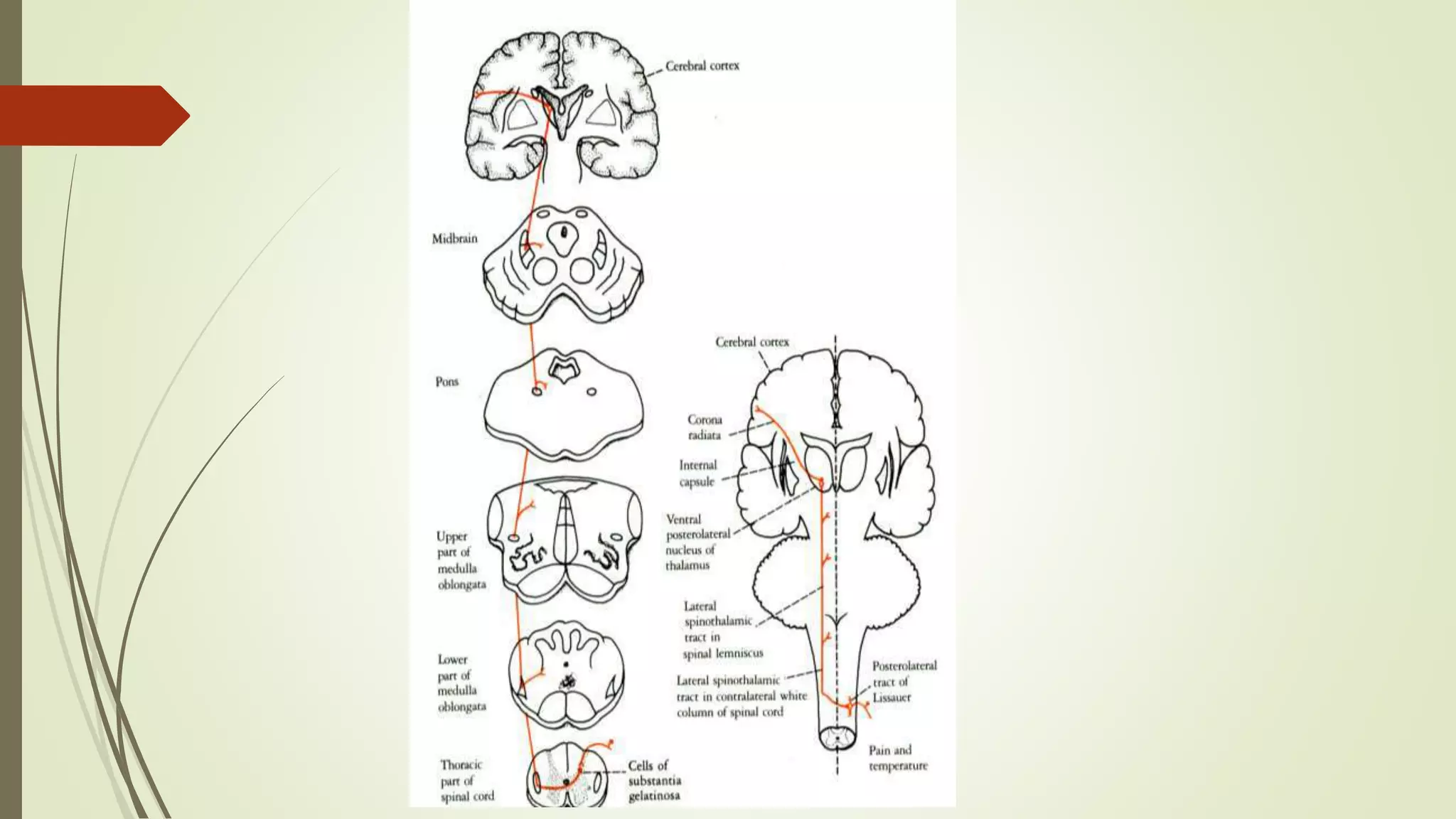
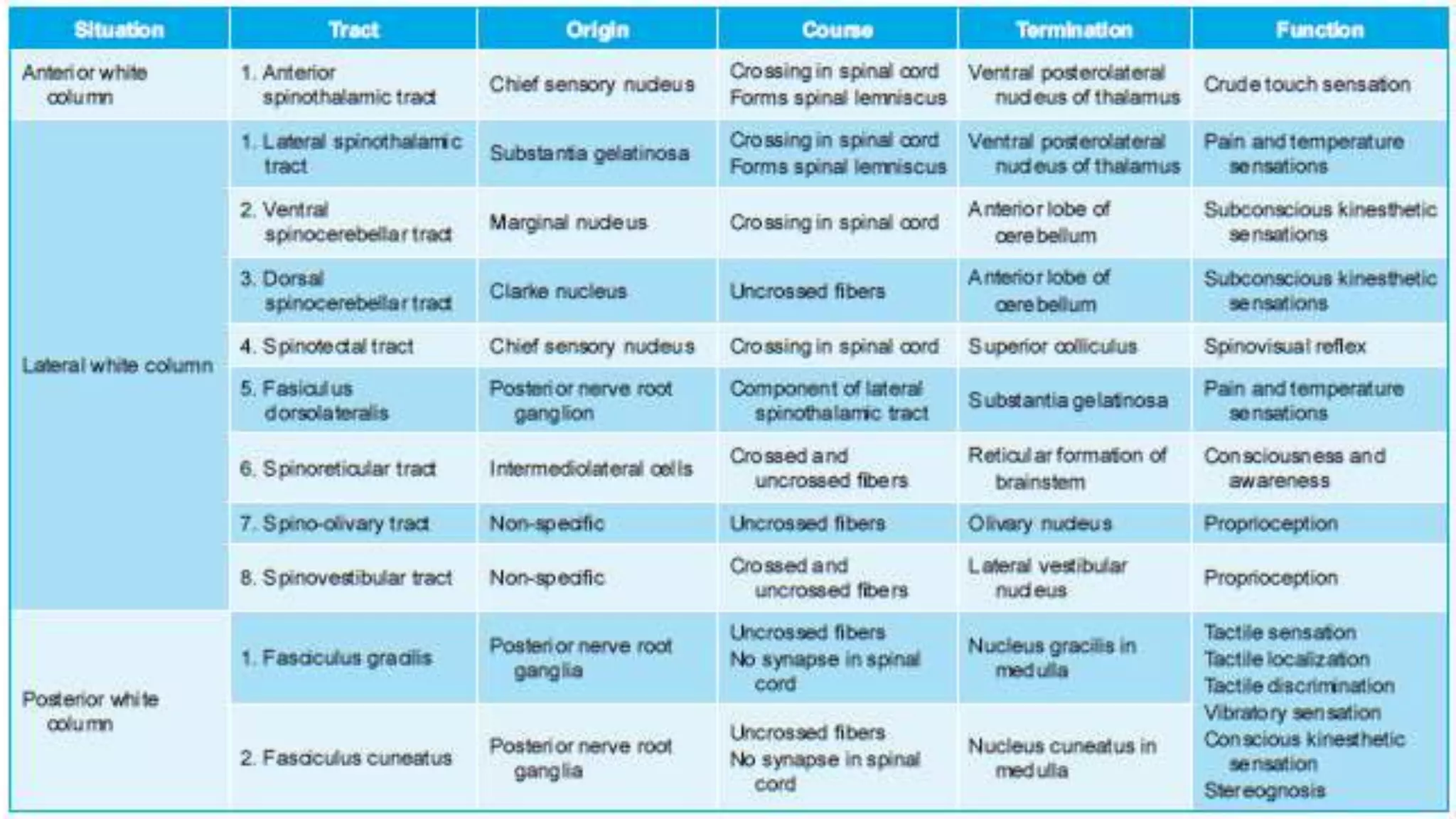
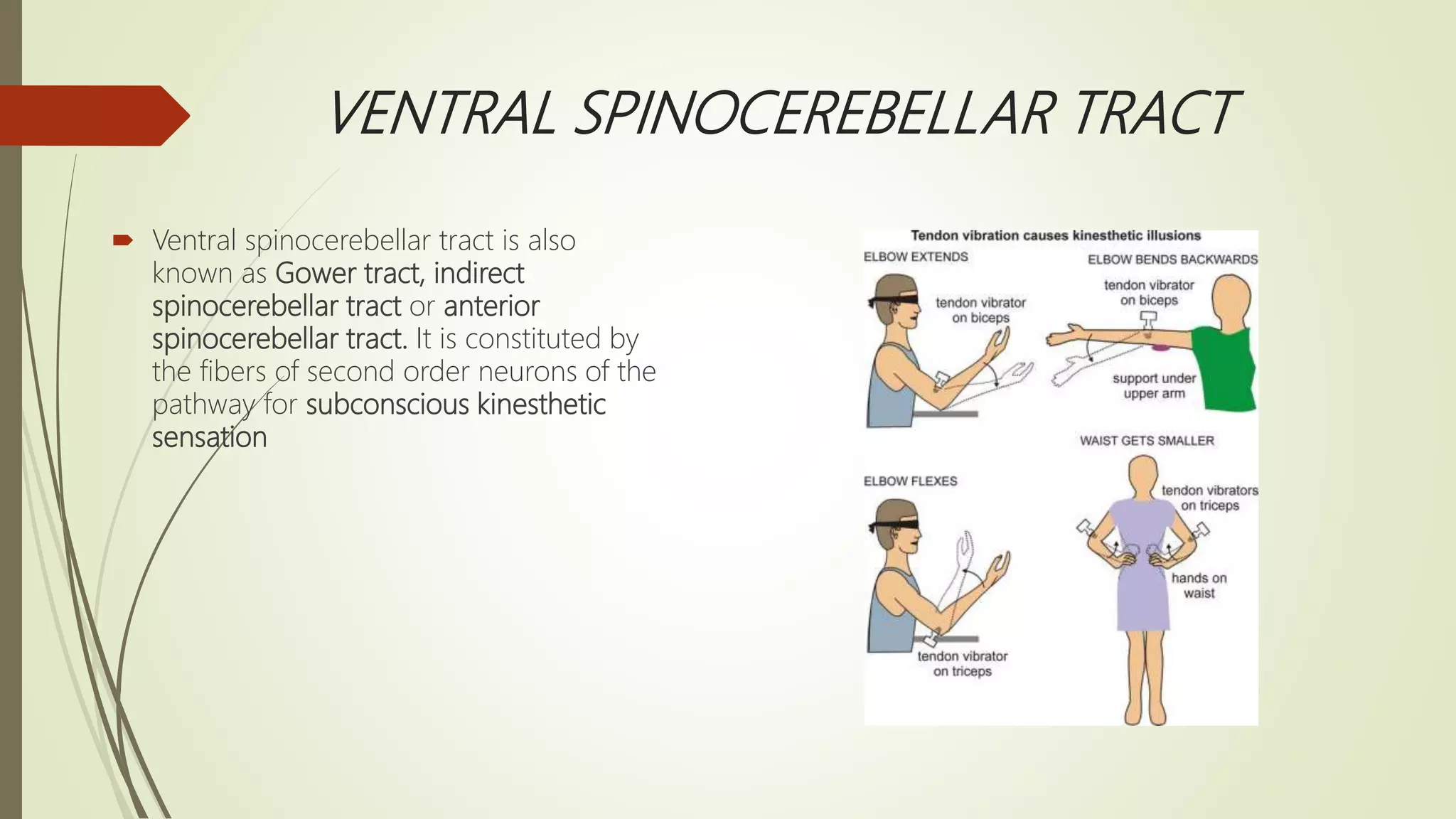

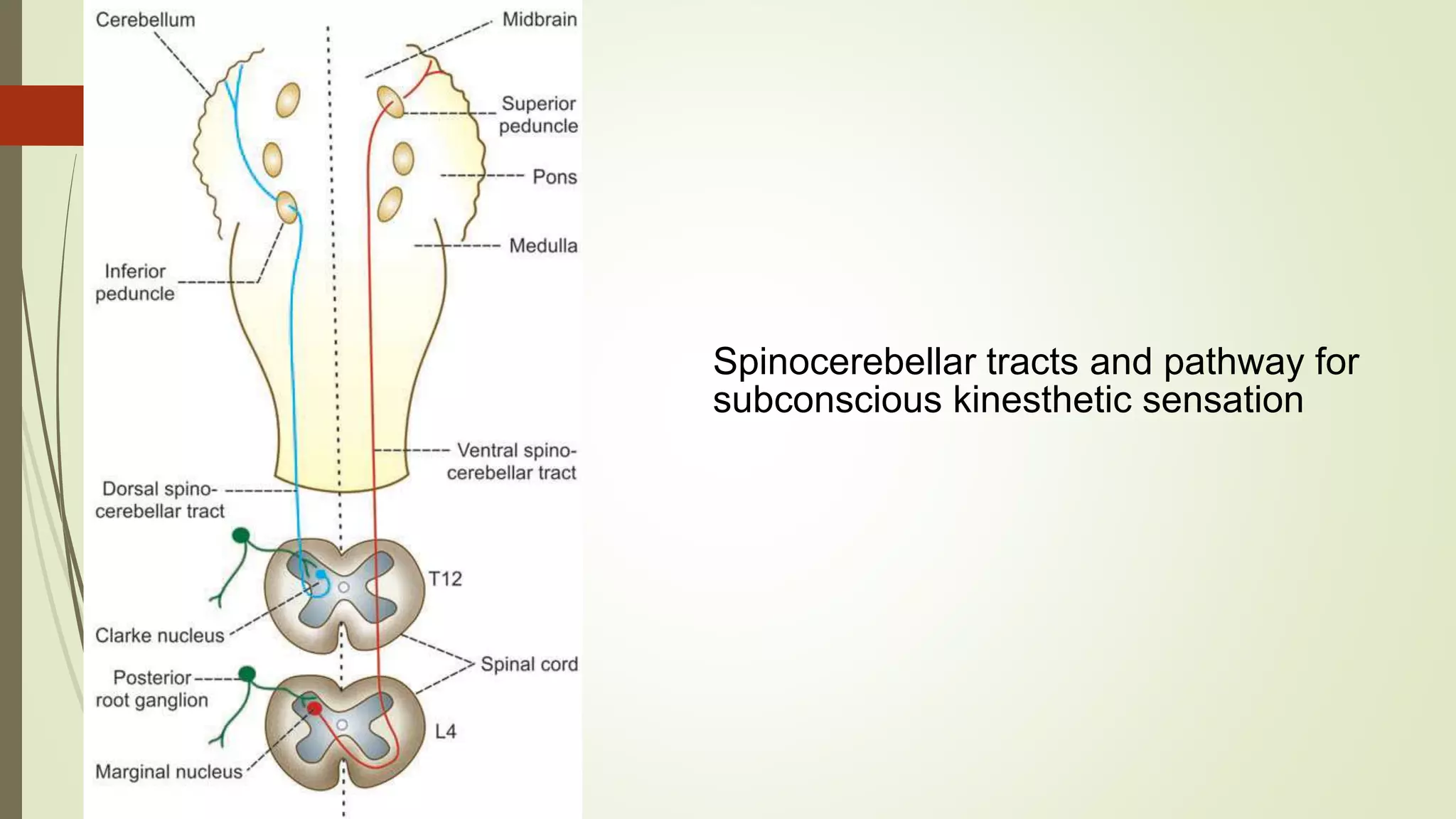

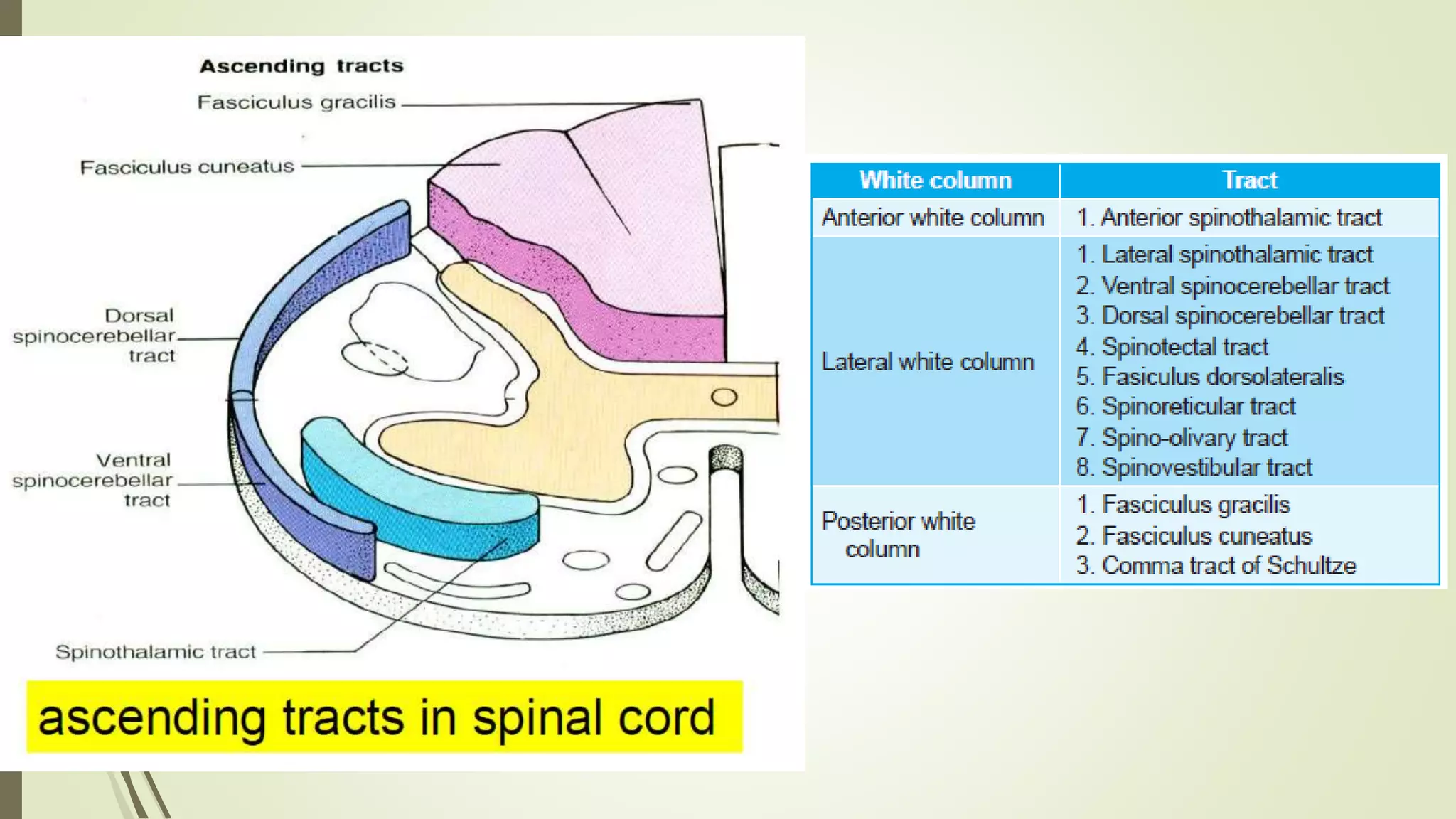

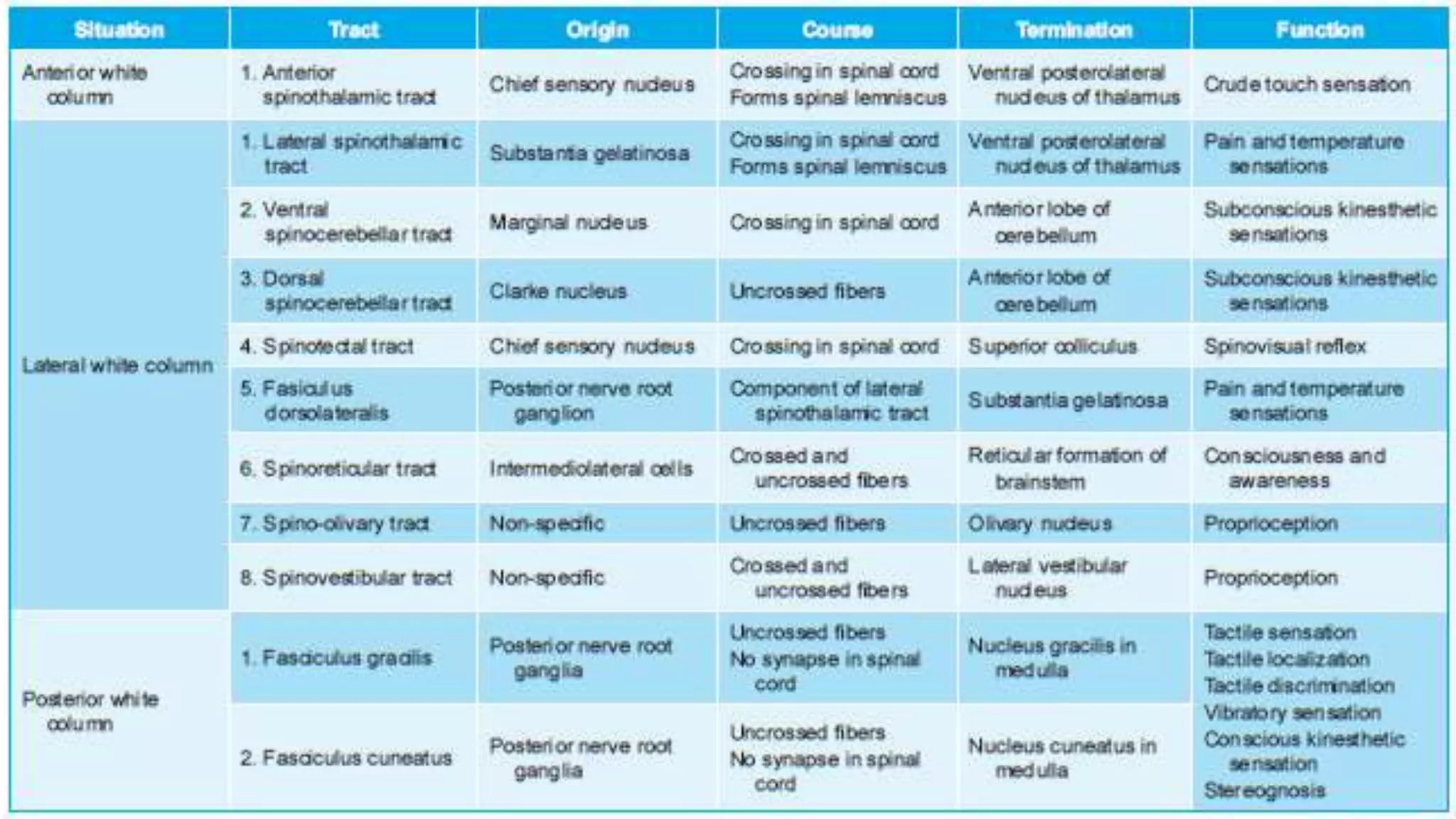











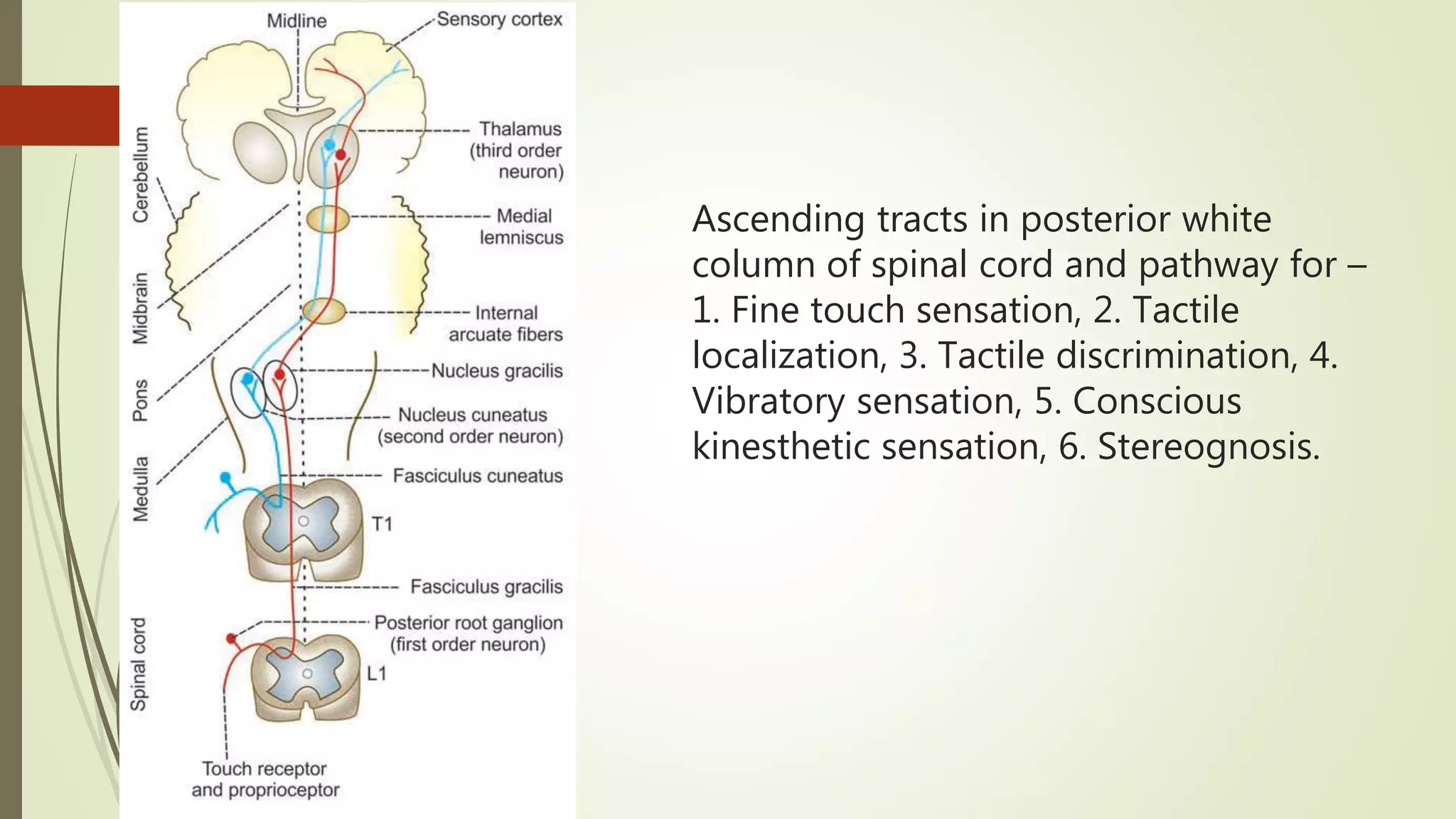


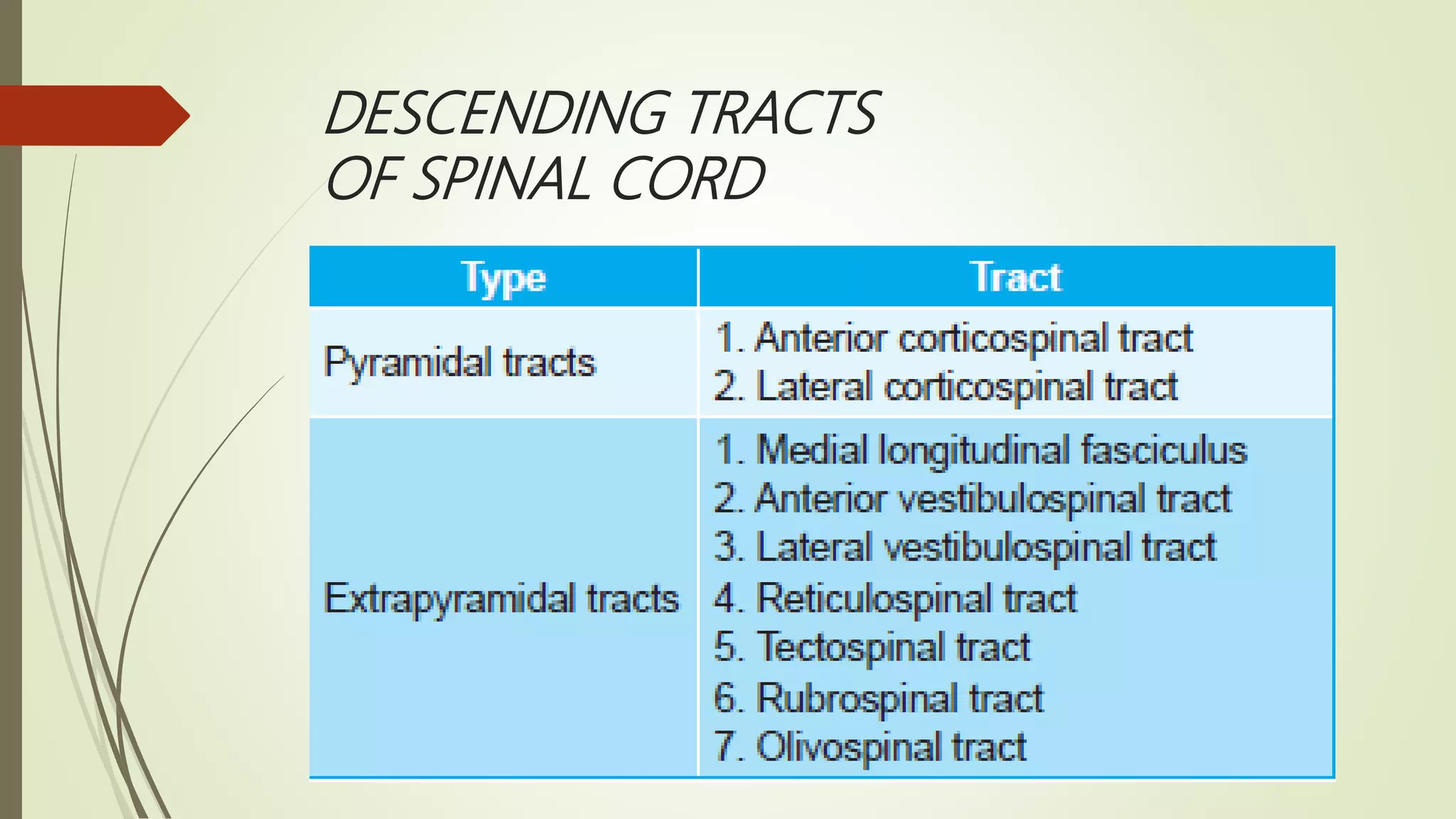
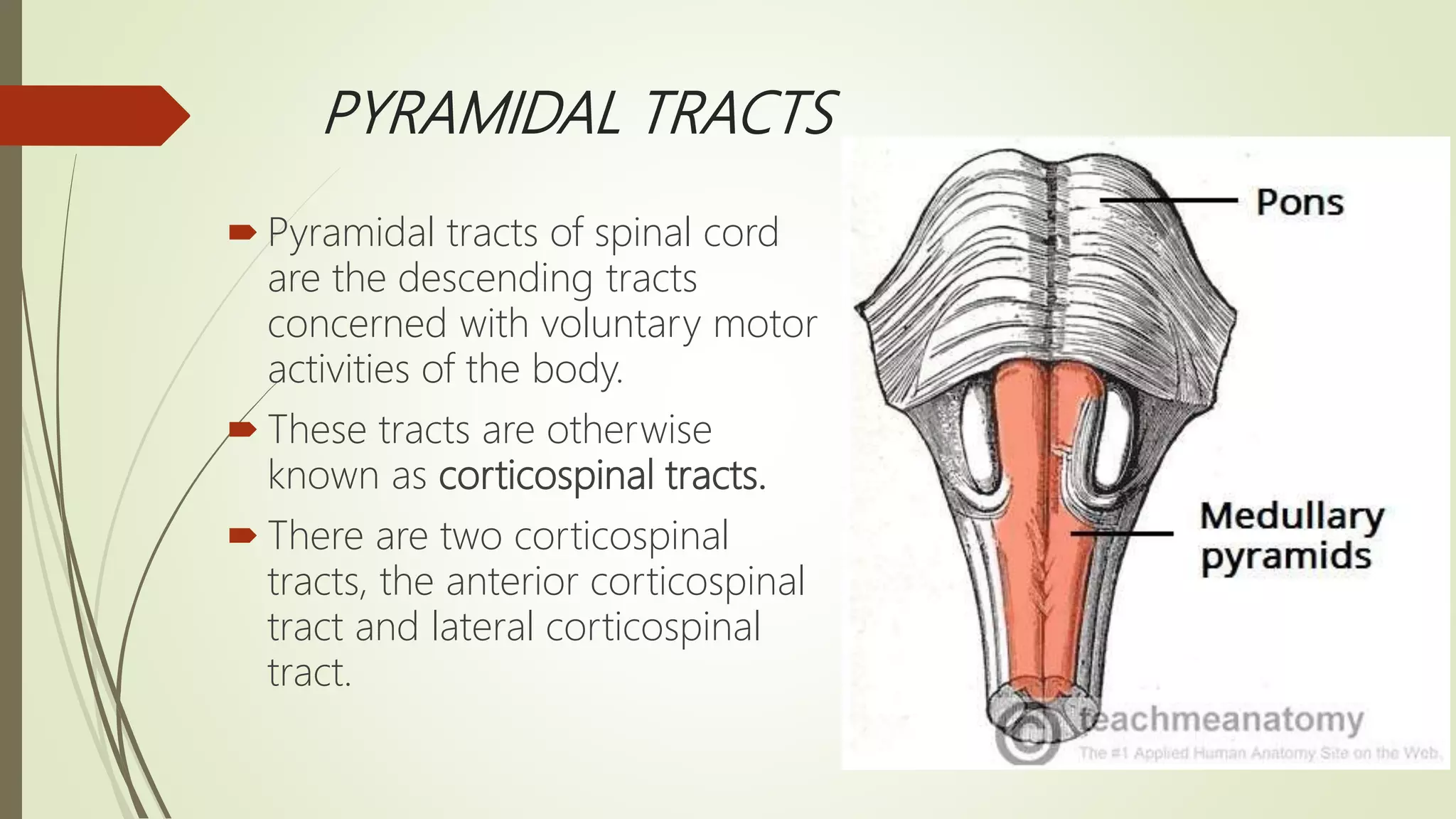
































































The document discusses the ascending and descending spinal pathways. It describes the short and long tracts of the spinal cord. The long tracts include ascending tracts that carry sensory impulses from the spinal cord to the brain, and descending tracts that carry motor impulses from the brain to the spinal cord. It provides details on three major ascending tracts - the anterior spinothalamic tract, lateral spinothalamic tract, and ventral spinocerebellar tract. It explains the origin, course, termination and functions of these tracts. The document also describes the dorsal spinocerebellar tract and its role in proprioception.























































































