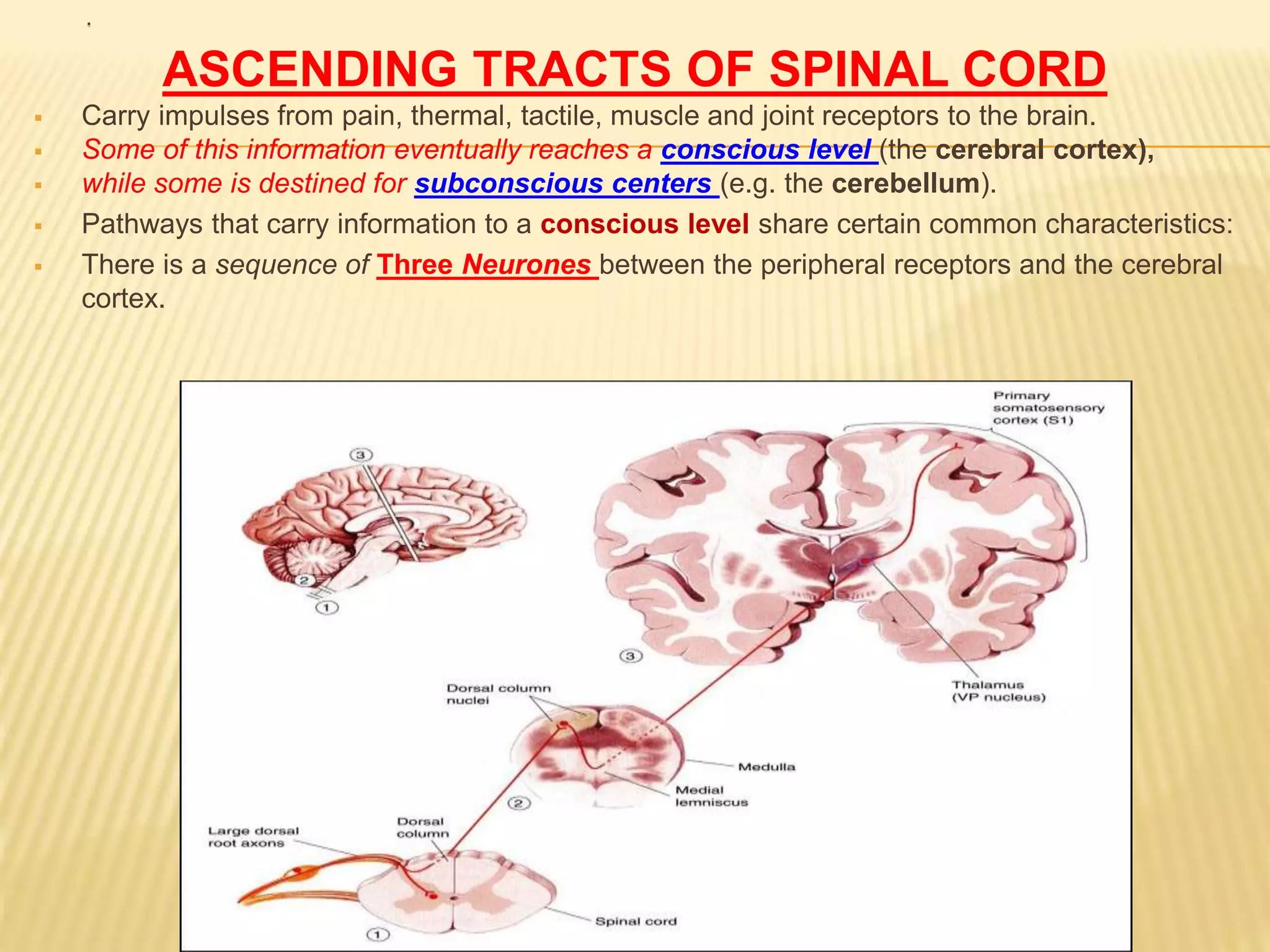
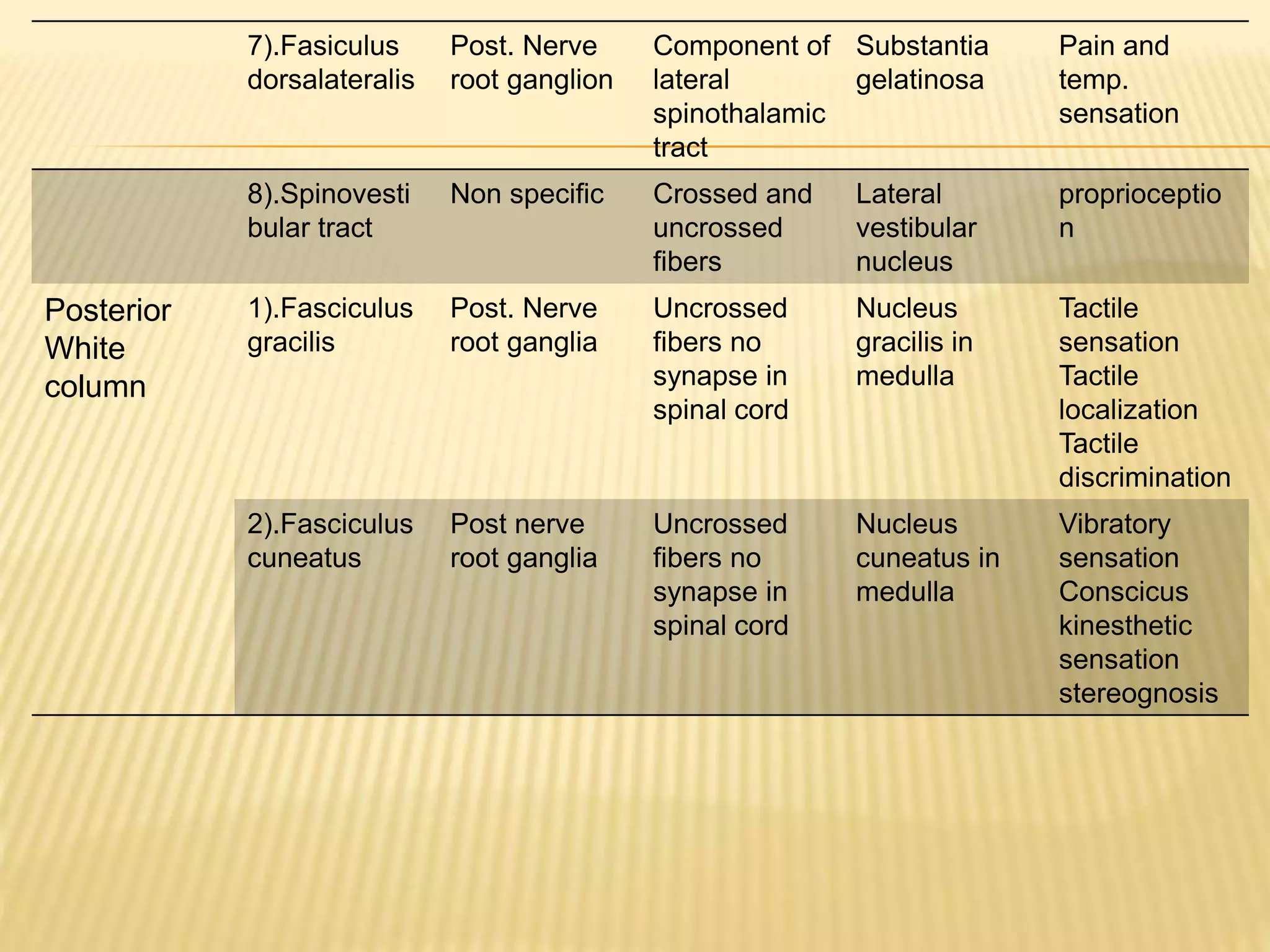
The document provides information on the ascending tracts of the spinal cord, which carry sensory information from the periphery to the brain. It discusses the three neuron pathway and lists eight major ascending tracts - the posterior white column tracts (fasciculus gracilis and cuneatus), lateral spinothalamic tract, anterior spinothalamic tract, spinocerebellar tracts, spinotectal tract, spino-olivary tract, and spinoreticular tract. Each tract is described in terms of its origin, course, termination, and function in sensory processing and perception. Lesions to different tracts can result in loss of specific sensory modalities.