Download to read offline





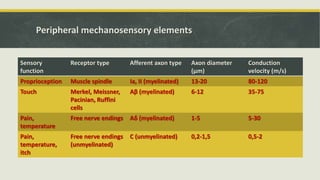

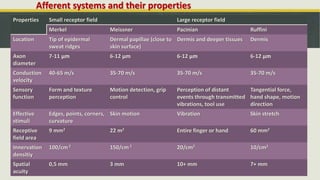

























The document discusses mechanosensation and the somatosensory system. It describes the basic organization, including labeled lines for different sensory functions. It outlines the peripheral mechanosensory elements like various receptor types, their locations and functions. It details the pathways for mechanosensation from the post-cranial body and face, including the dorsal column medial lemniscus system and trigeminal lemniscus pathway. It also discusses proprioception, muscle spindles, golgi tendon organs, and areas of the cortex involved in somatosensory processing.





















![Introduction to the nervous system and nerve tissue[1]](https://cdn.slidesharecdn.com/ss_thumbnails/may2013introductiontothenervoussystemandnervetissue1-150530193624-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)





























































