






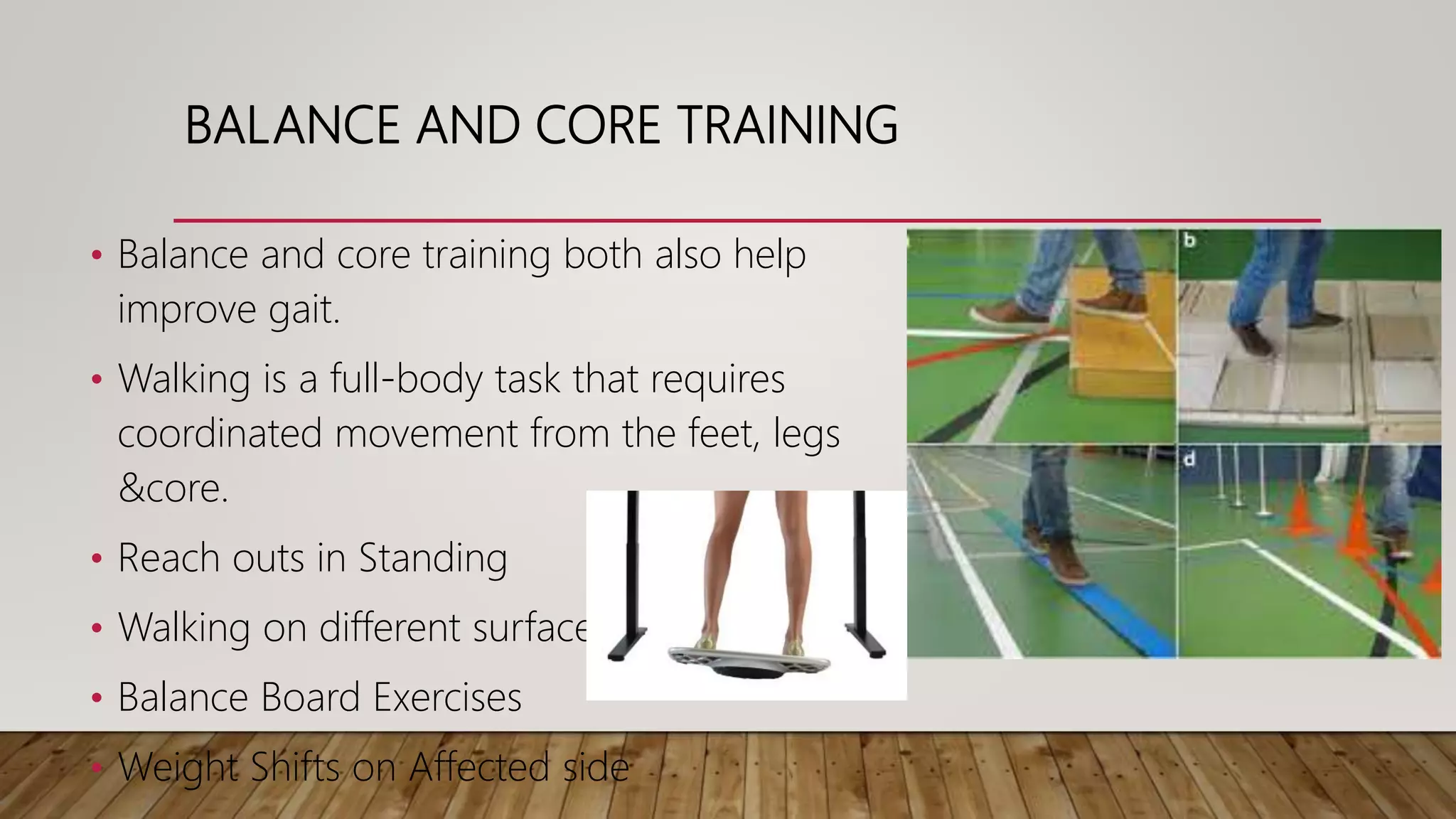
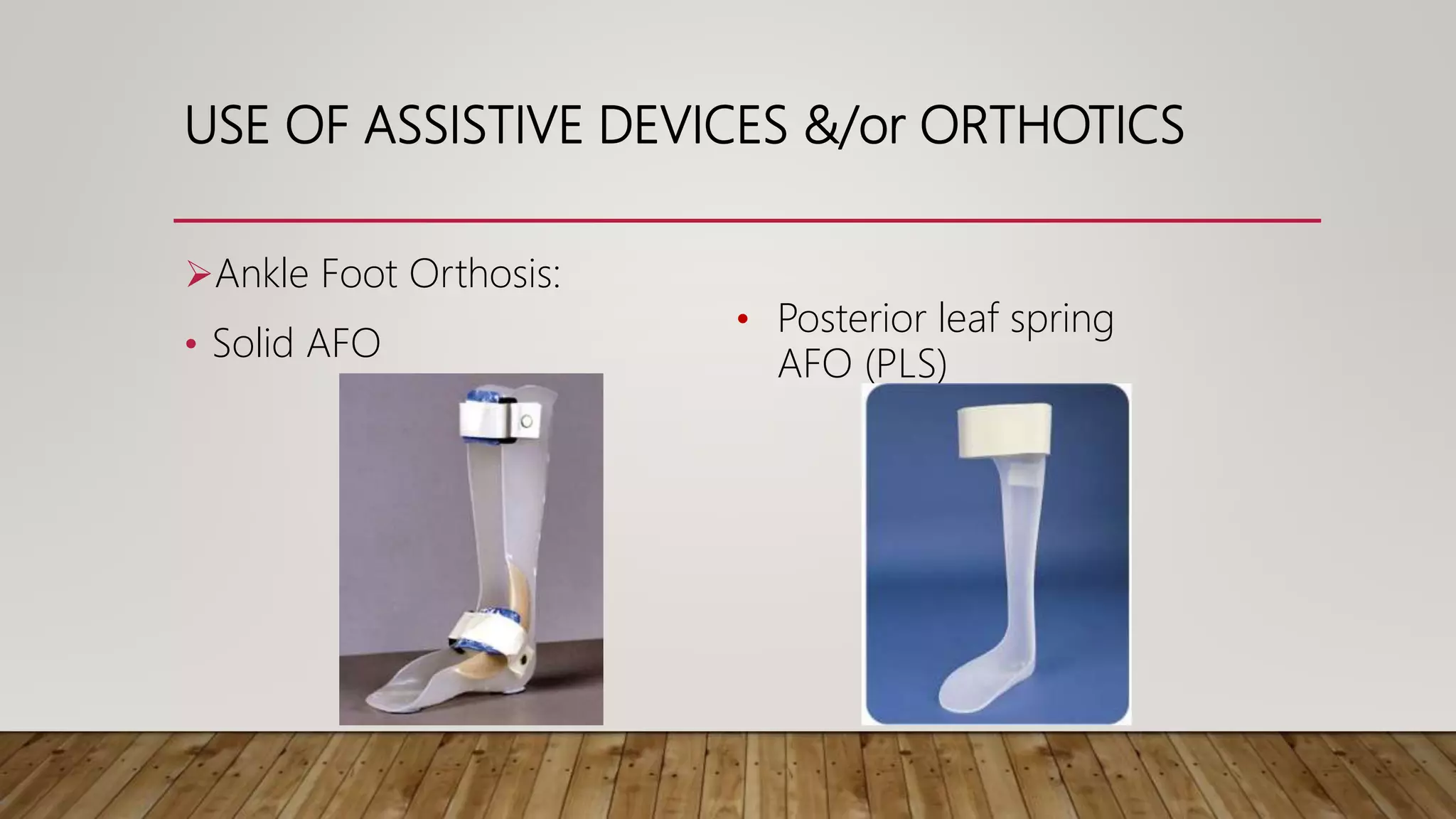

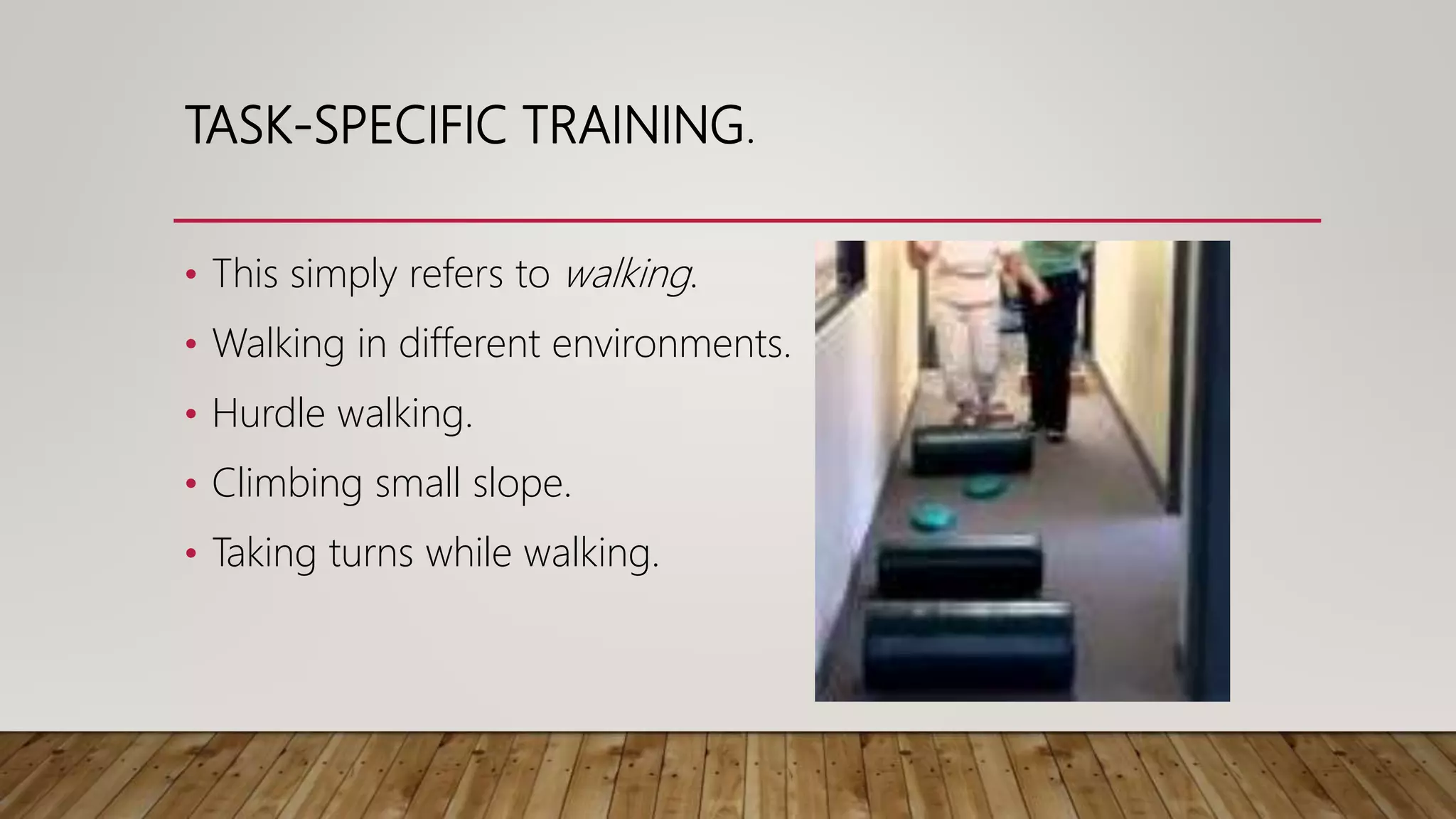

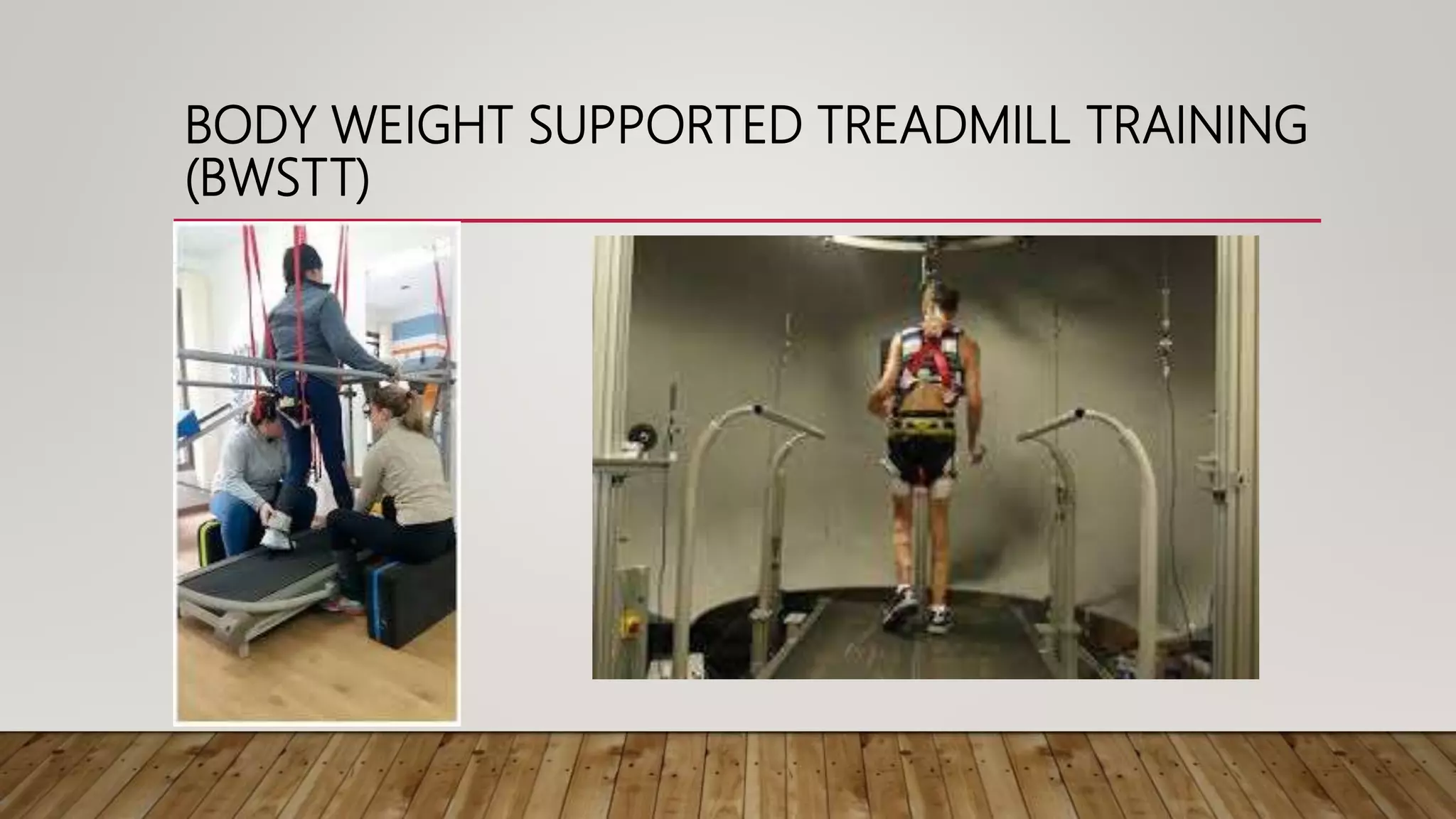





The document discusses hemiplegic gait rehabilitation, detailing the characteristics of hemiplegic gait, including circumduction and reduced leg movement. It outlines various rehabilitation methods such as traditional and high-tech approaches, including gait training exercises, balance training, and the use of assistive devices. Emphasis is placed on the benefits of consistent rehabilitation to improve stability and prevent falls after stroke.






















































































