Downloaded 66 times









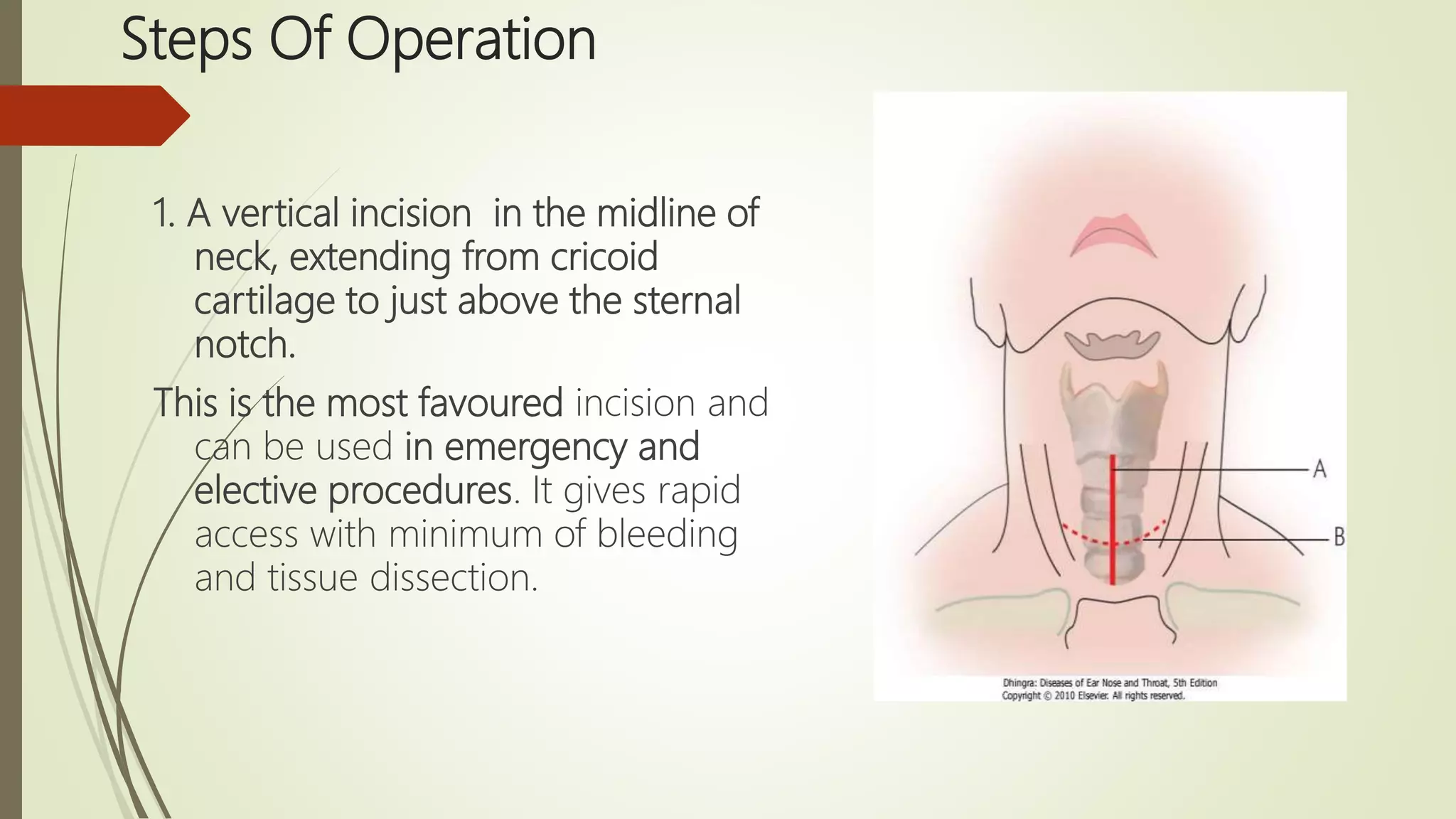











Tracheostomy has been performed since ancient times to relieve airway obstruction. The first documented successful tracheostomy was performed in the 15th century by Brasovala. Tracheostomies are now used to provide an alternative airway, remove secretions, assist ventilation, and protect the airway during procedures involving the mouth or larynx. The procedure involves making an incision in the trachea and inserting a tracheostomy tube. Care must be taken when performing tracheostomies in children due to the small size of the trachea. Complications can occur during or after the procedure such as bleeding, tube displacement or blockage, and long term issues like stenosis.



































































