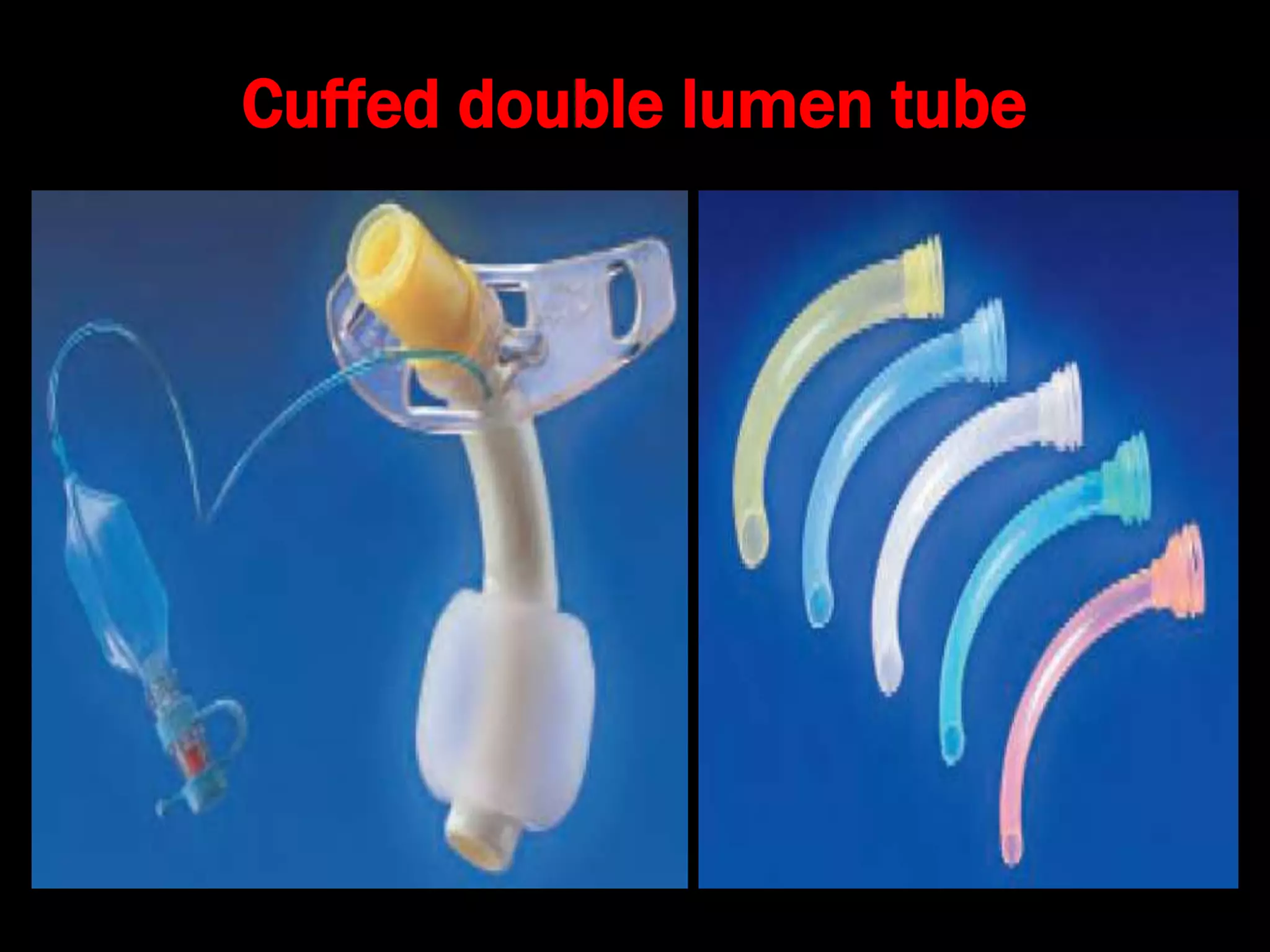
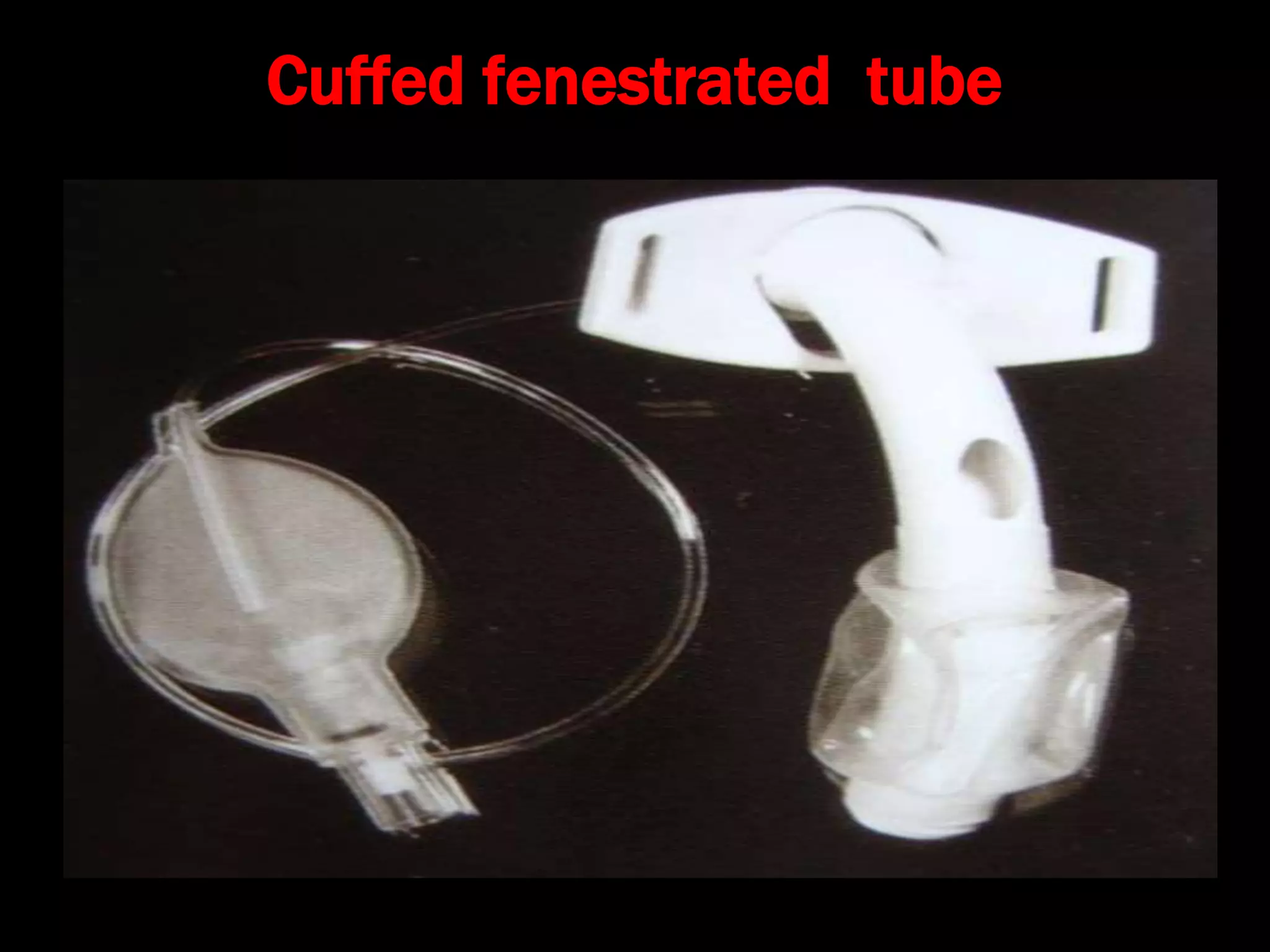
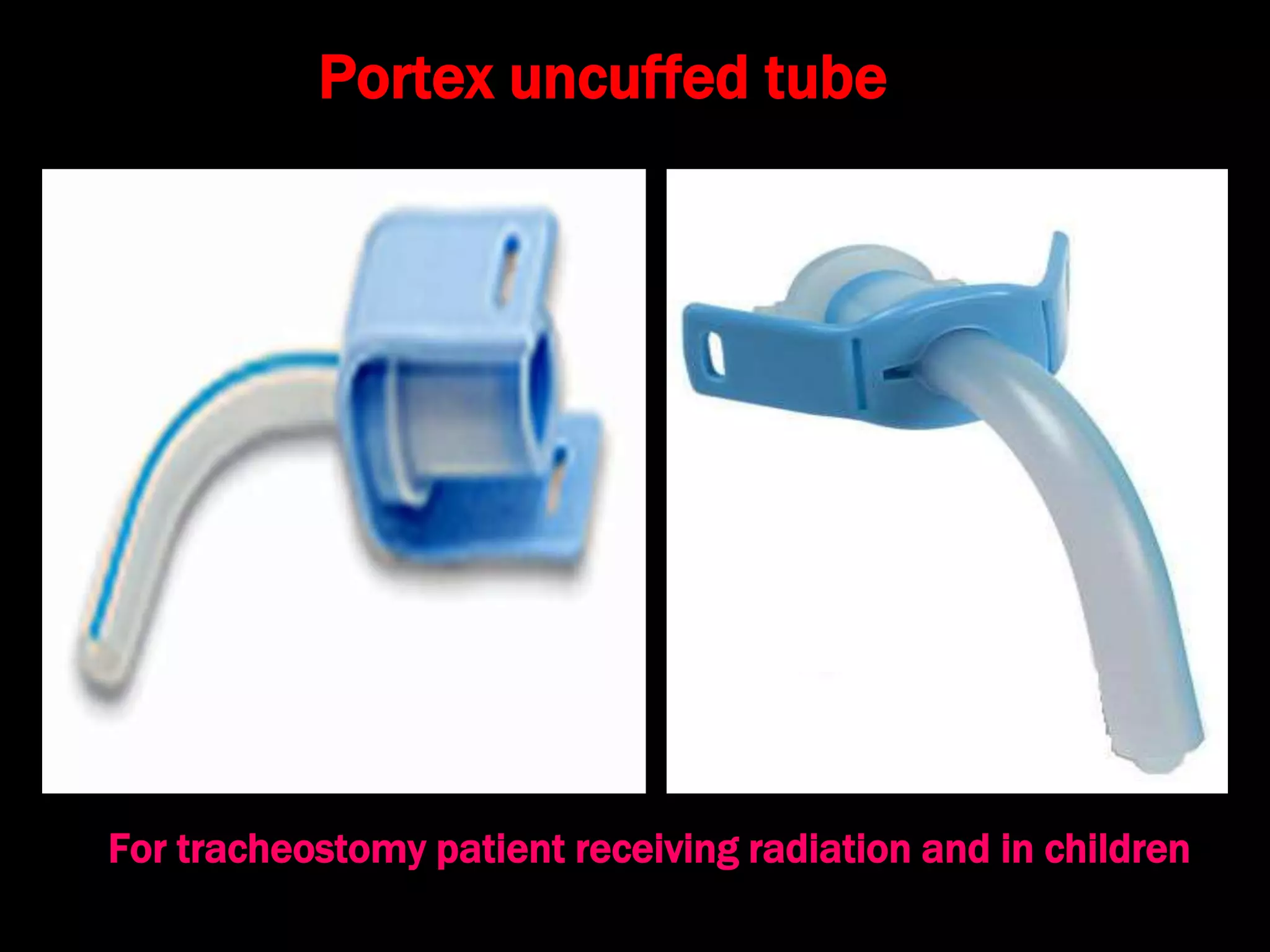
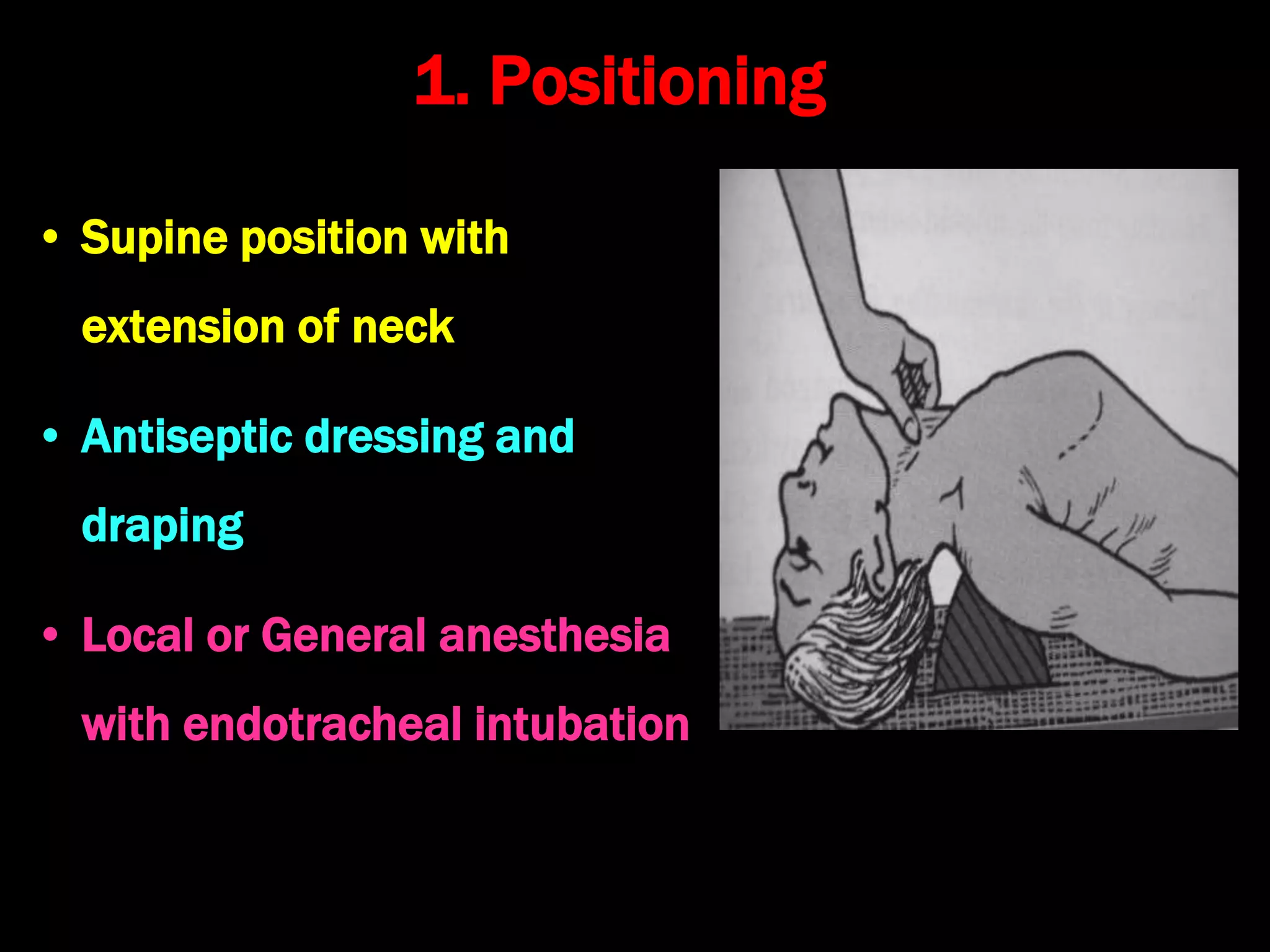
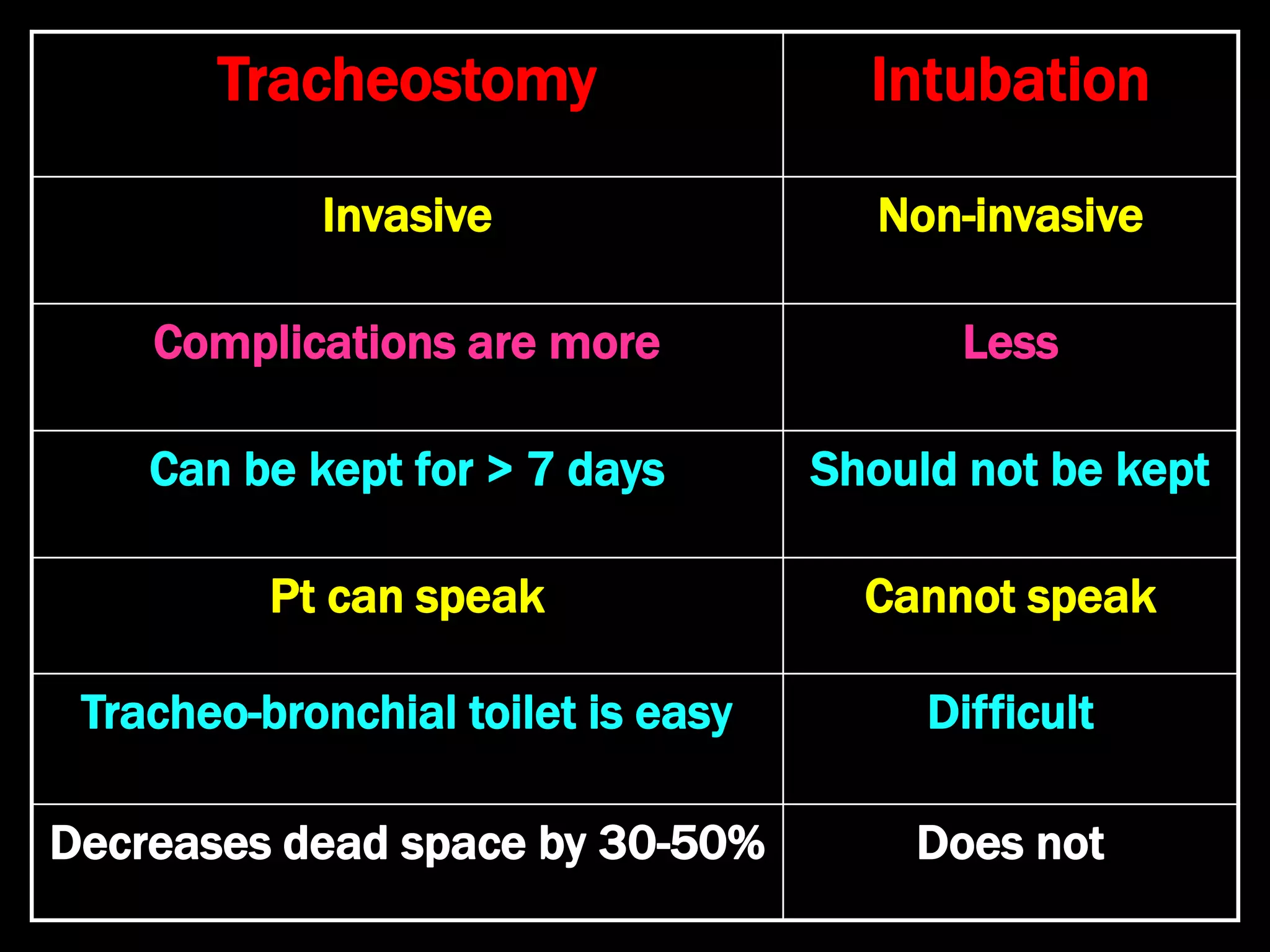
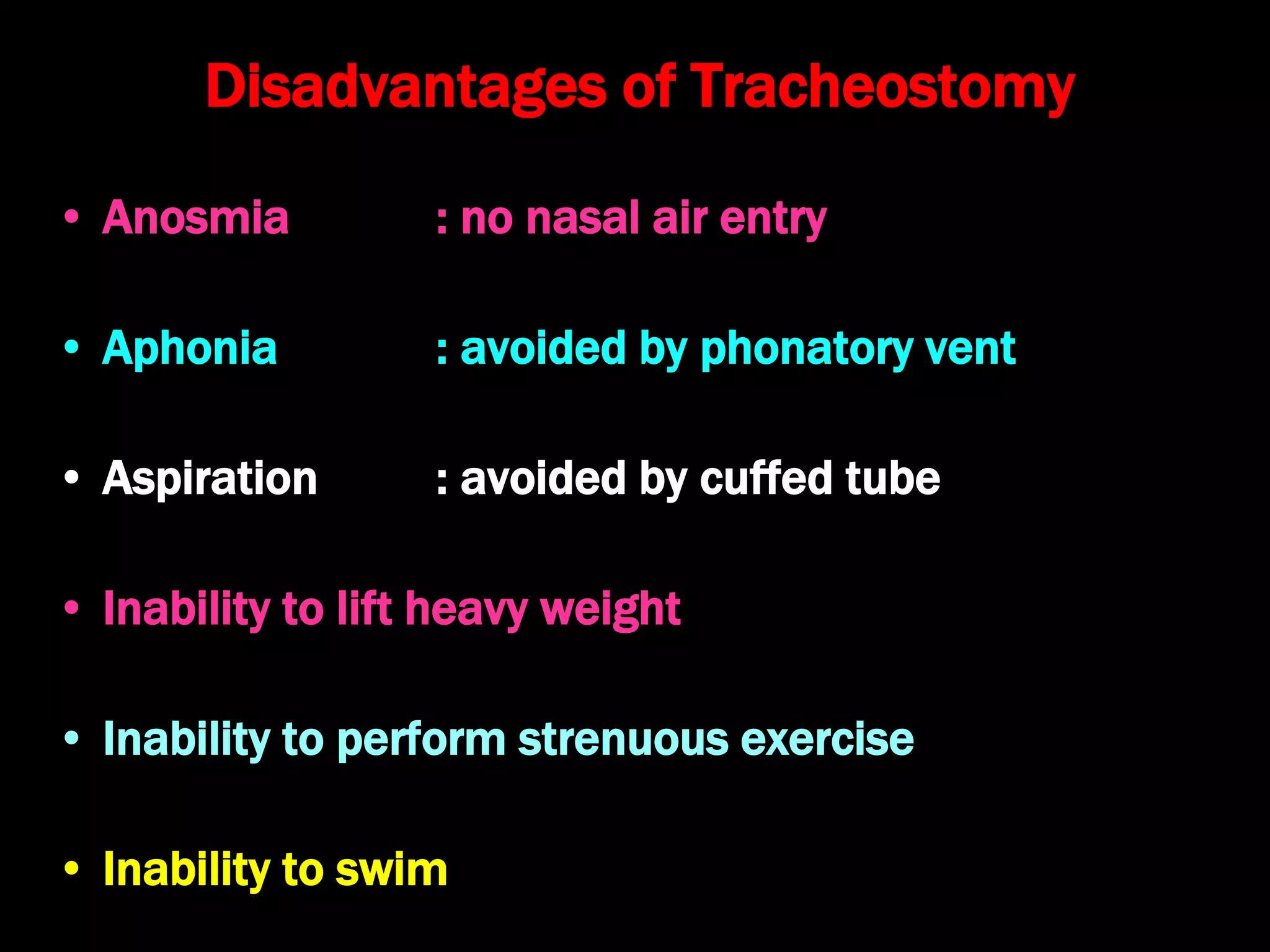
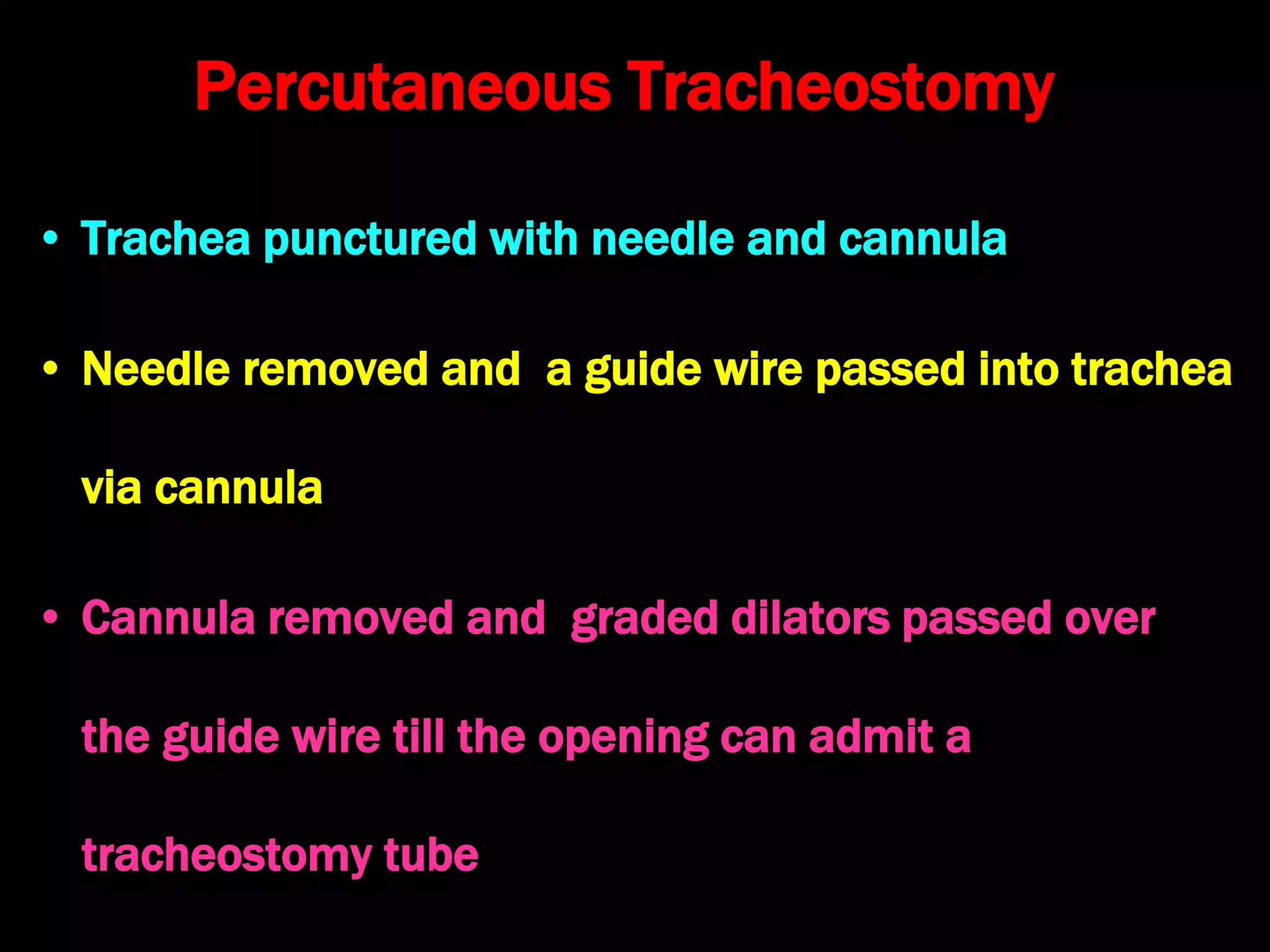
Tracheostomy is a surgical procedure to create an opening into the trachea through the neck. It has evolved from a feared procedure to a commonly performed one for various airway issues and respiratory conditions. The document describes the history, indications, types of tracheostomy tubes used, procedure steps, potential complications and advantages/disadvantages. A tracheostomy aims to relieve upper airway obstruction and facilitate respiratory management but requires long term care and has risks of complications if not performed correctly.