Downloaded 476 times

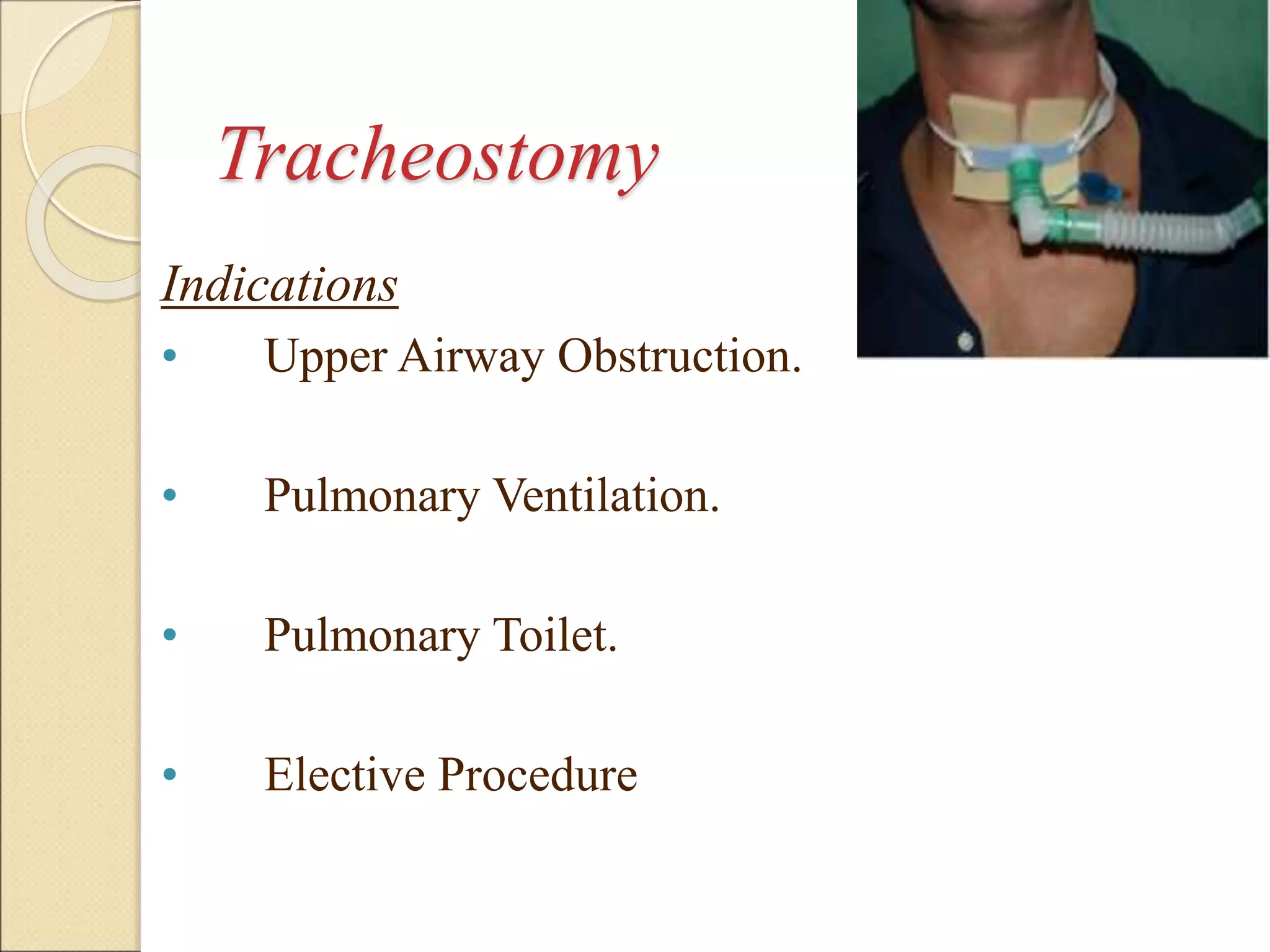

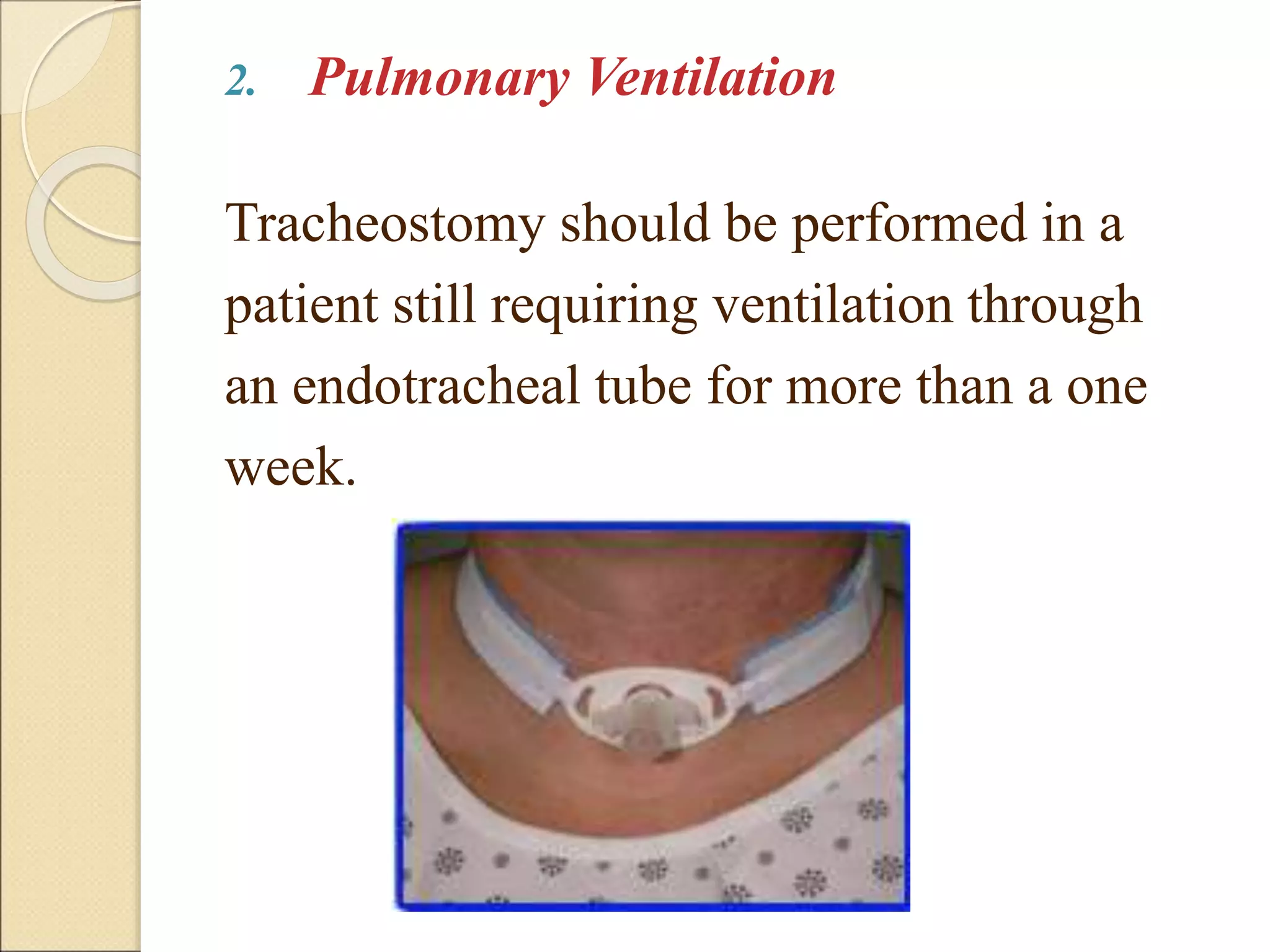


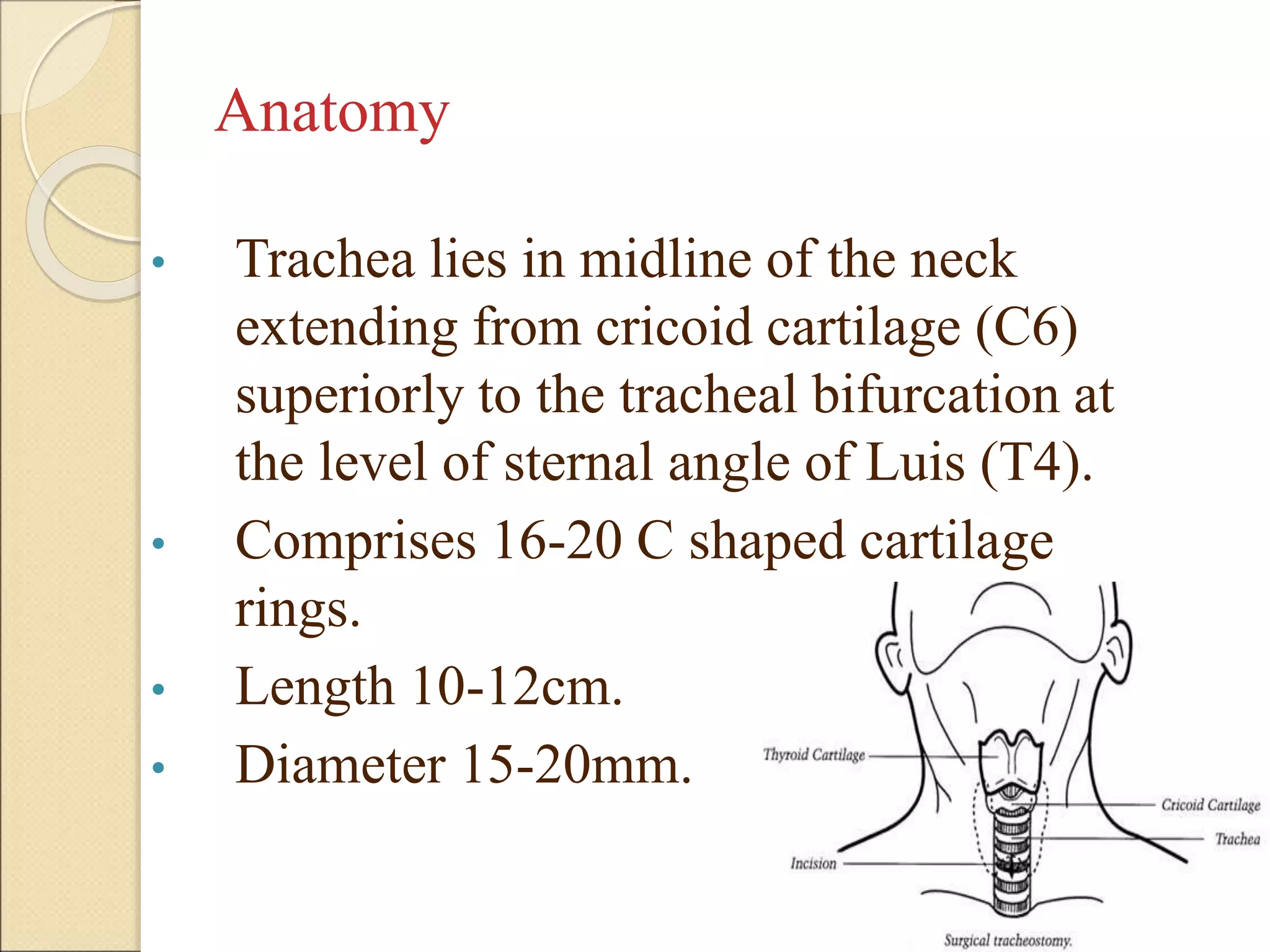






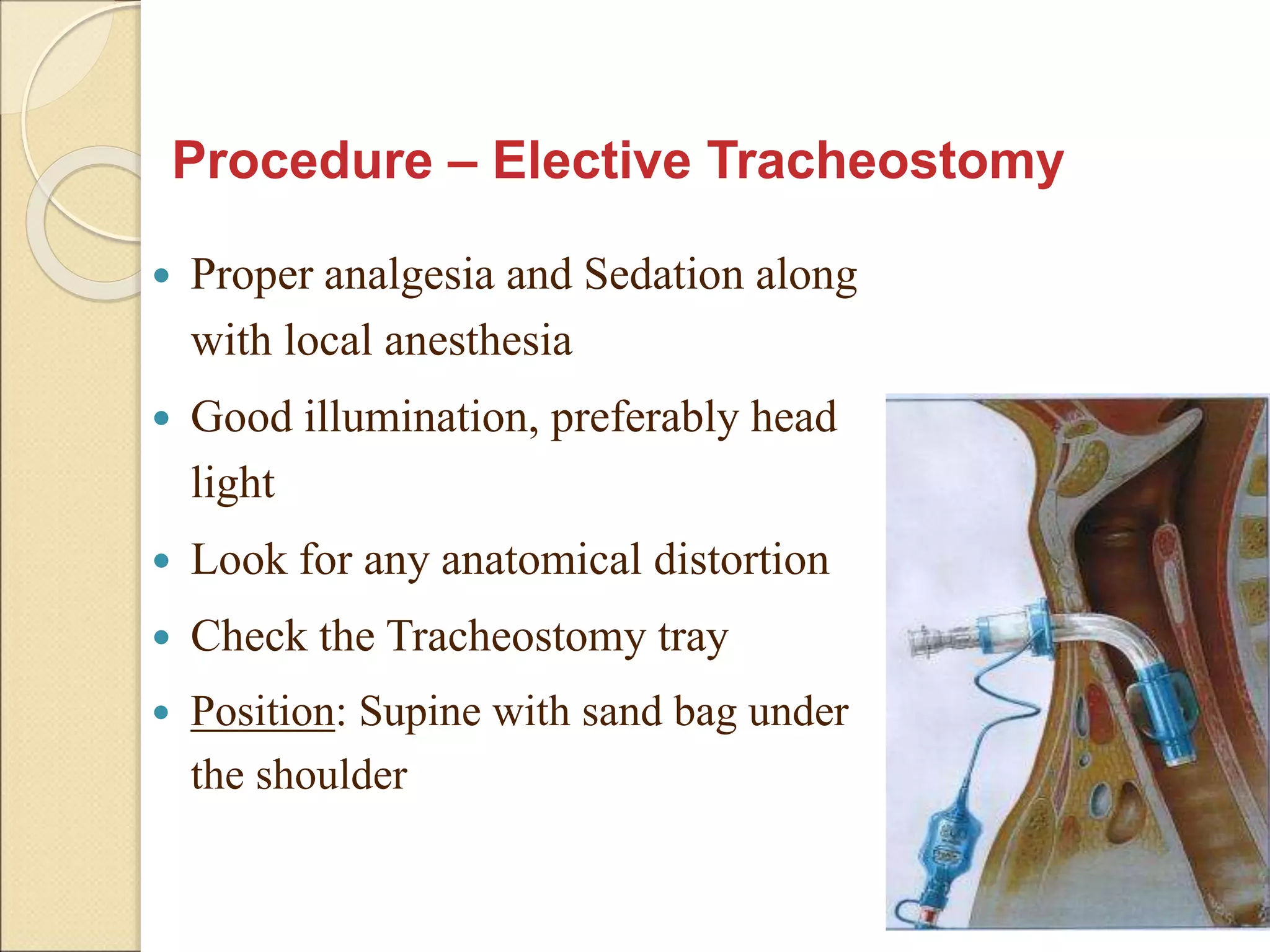




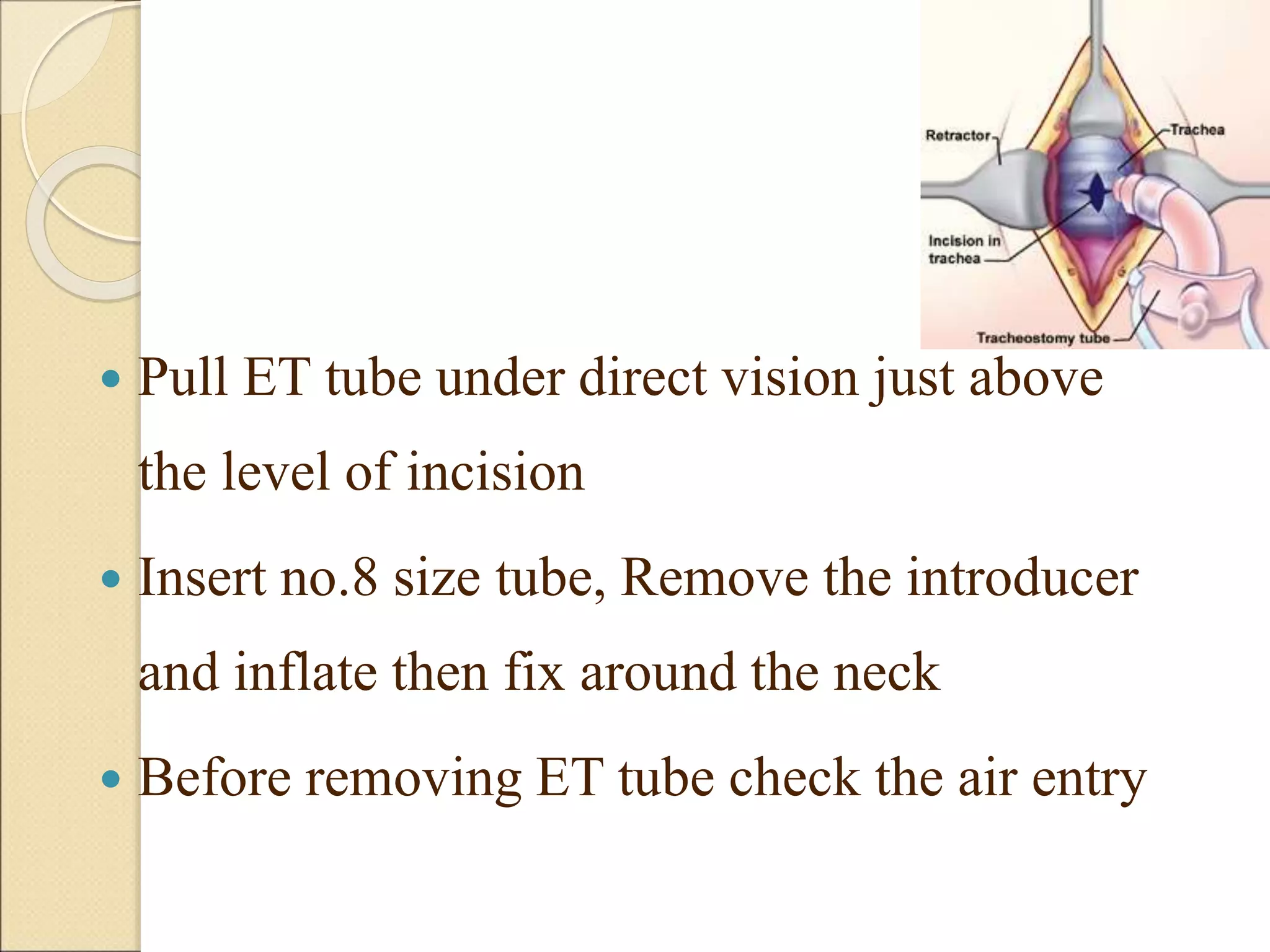

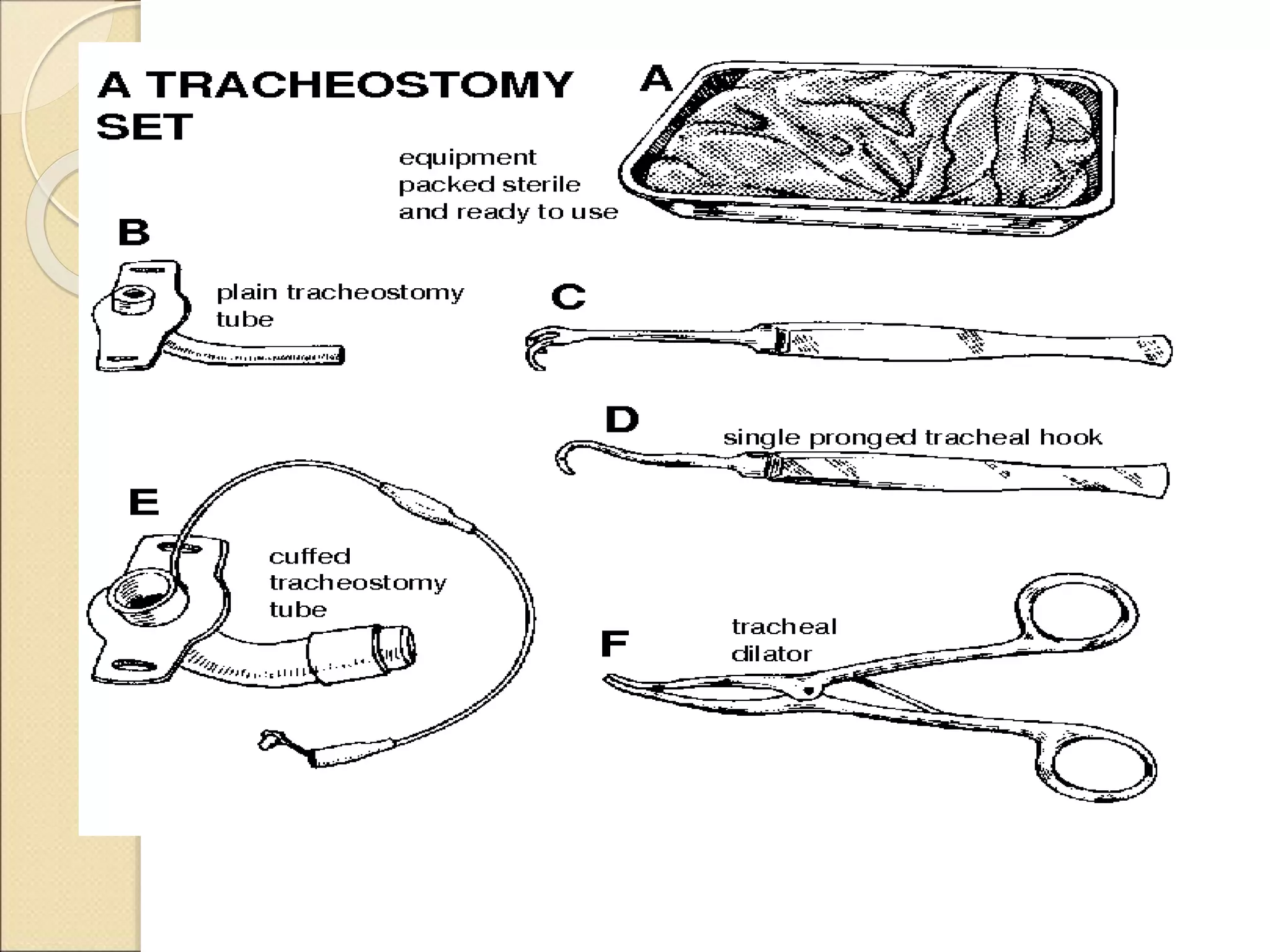




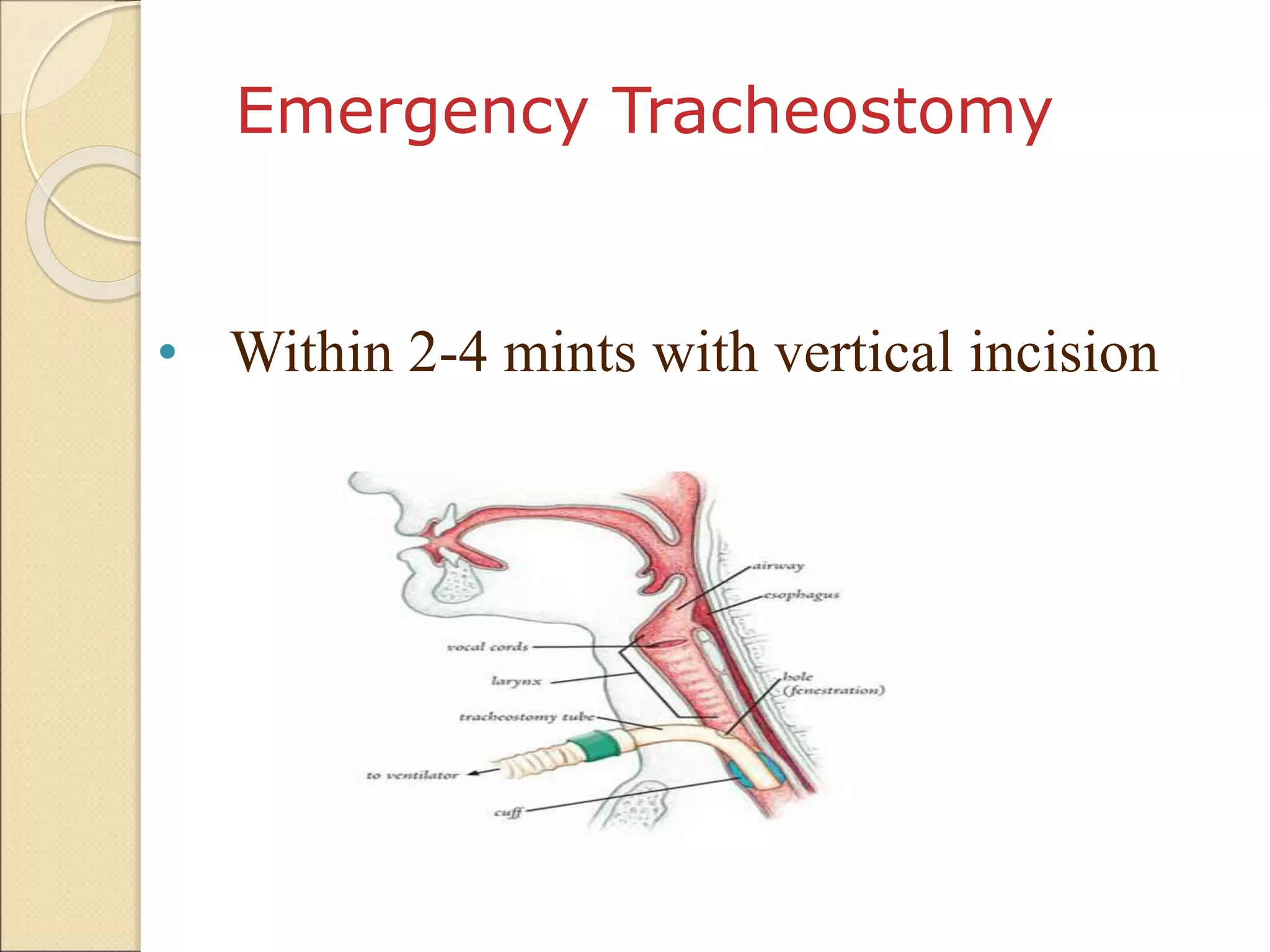


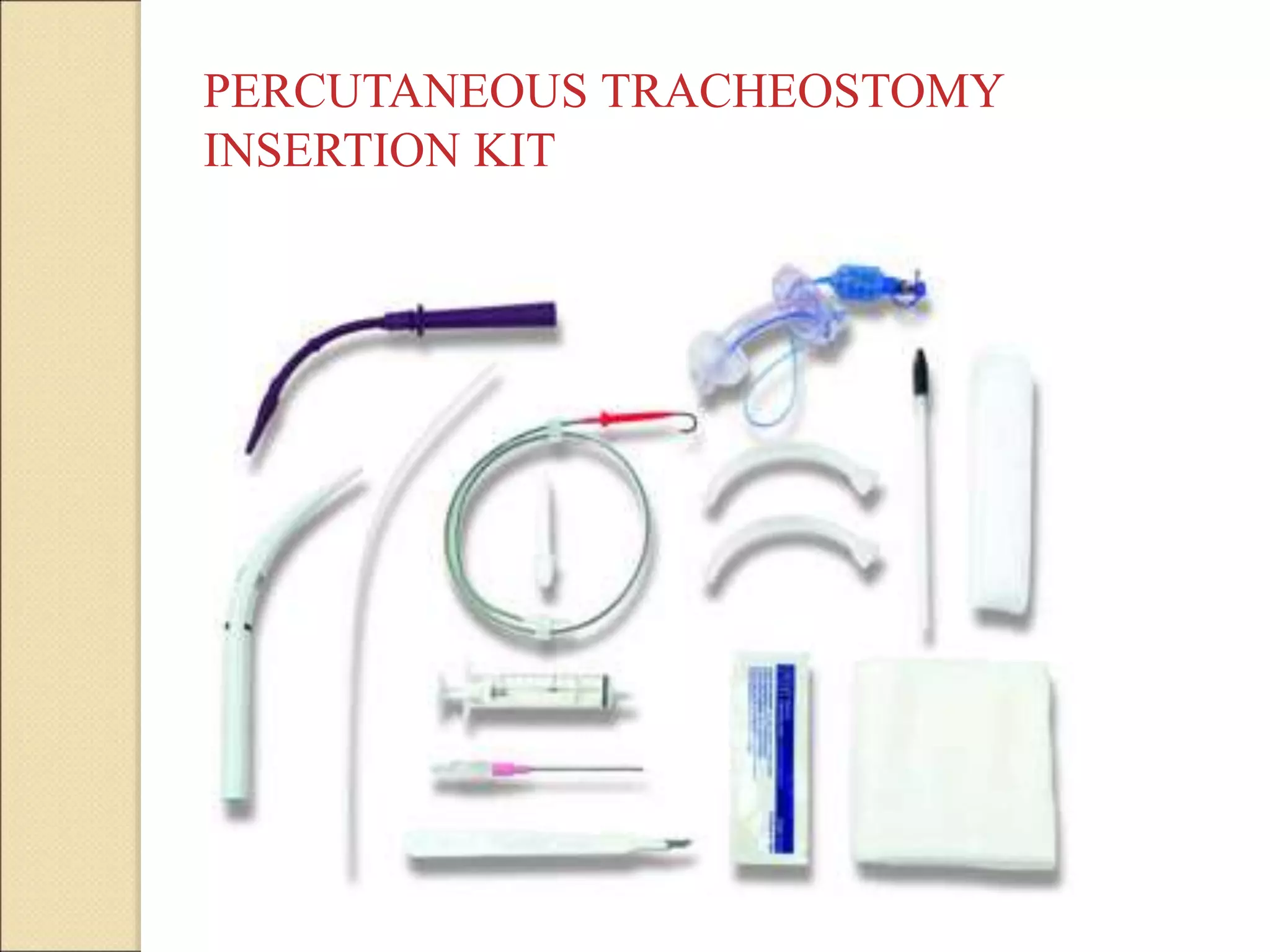



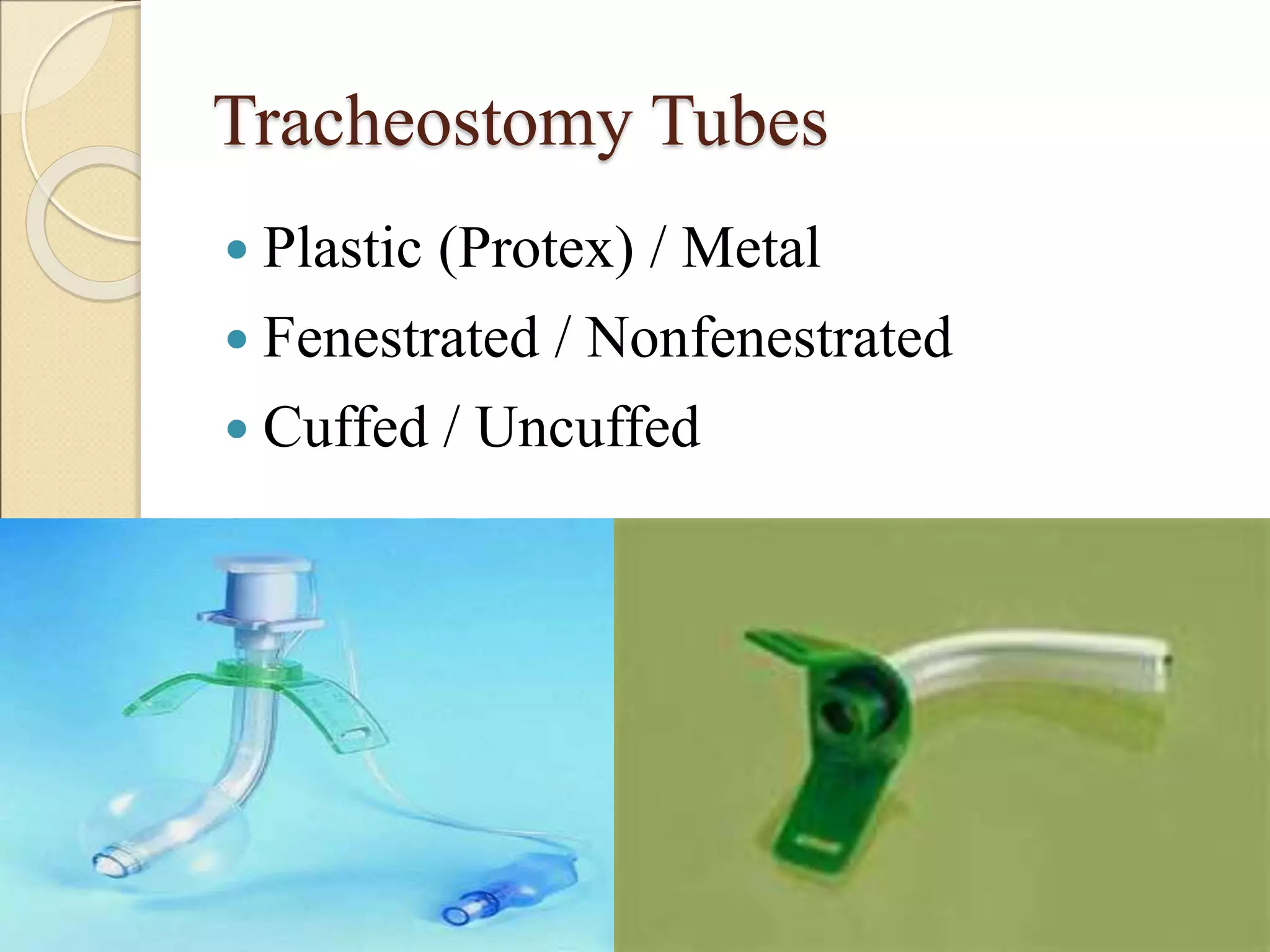



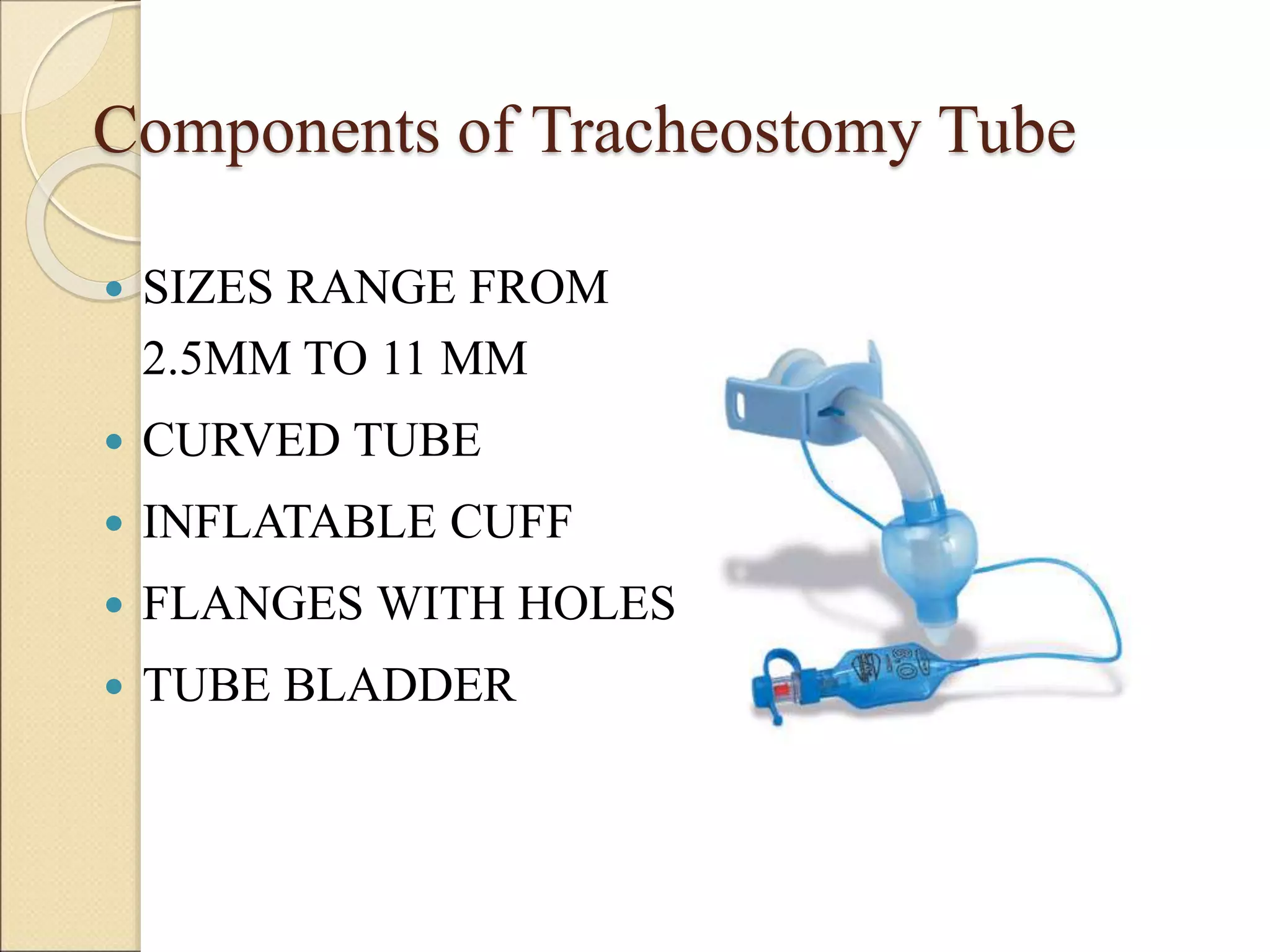



























A tracheostomy is a surgically created opening in the trachea (windpipe) through which a tracheostomy tube is inserted to provide an airway. There are several types including elective, emergency, and percutaneous tracheostomy. Indications include upper airway obstruction, need for prolonged mechanical ventilation, and inability to clear secretions. The procedure involves making an incision through the neck into the trachea and inserting a tracheostomy tube. Complications can include bleeding, infection, and tracheal stenosis. Ongoing care involves cleaning the stoma, suctioning secretions, monitoring tube placement, and providing nutrition and communication methods.























































































