
Downloaded 36 times

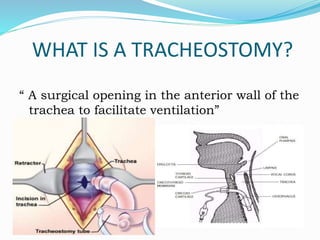






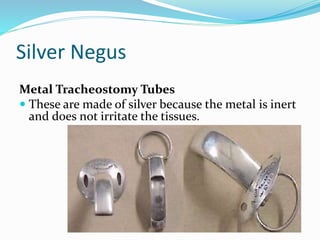

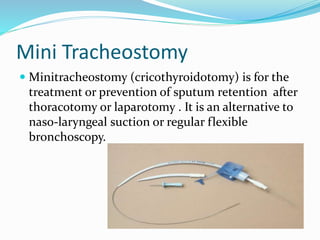










This document provides information about tracheostomies including: - A tracheostomy is a surgical opening in the front of the trachea to facilitate ventilation. - It has been performed since 100 BC and the first successful one was in the 15th century. - Tracheostomies can be temporary or permanent and use different types of tubes. - Indications include mechanical airway obstructions, infections, trauma, burns and impaired breathing. - Nursing care involves cleaning tubes, changing inner and outer tubes, caring for the stoma site, suctioning secretions, providing humidification and monitoring for complications. - The goal is to maintain an open airway and prevent infections while the patient he























































































