Download to read offline
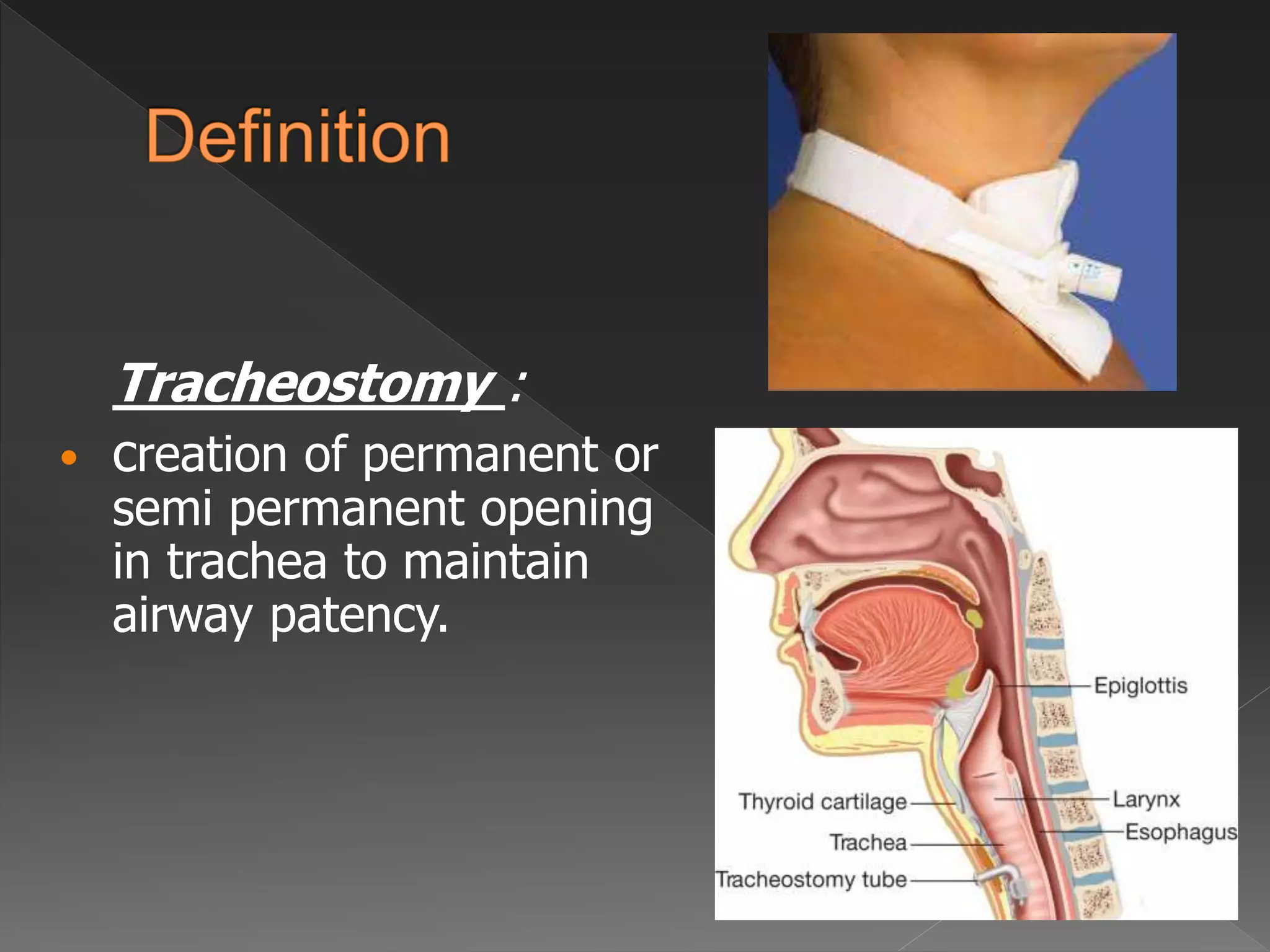

















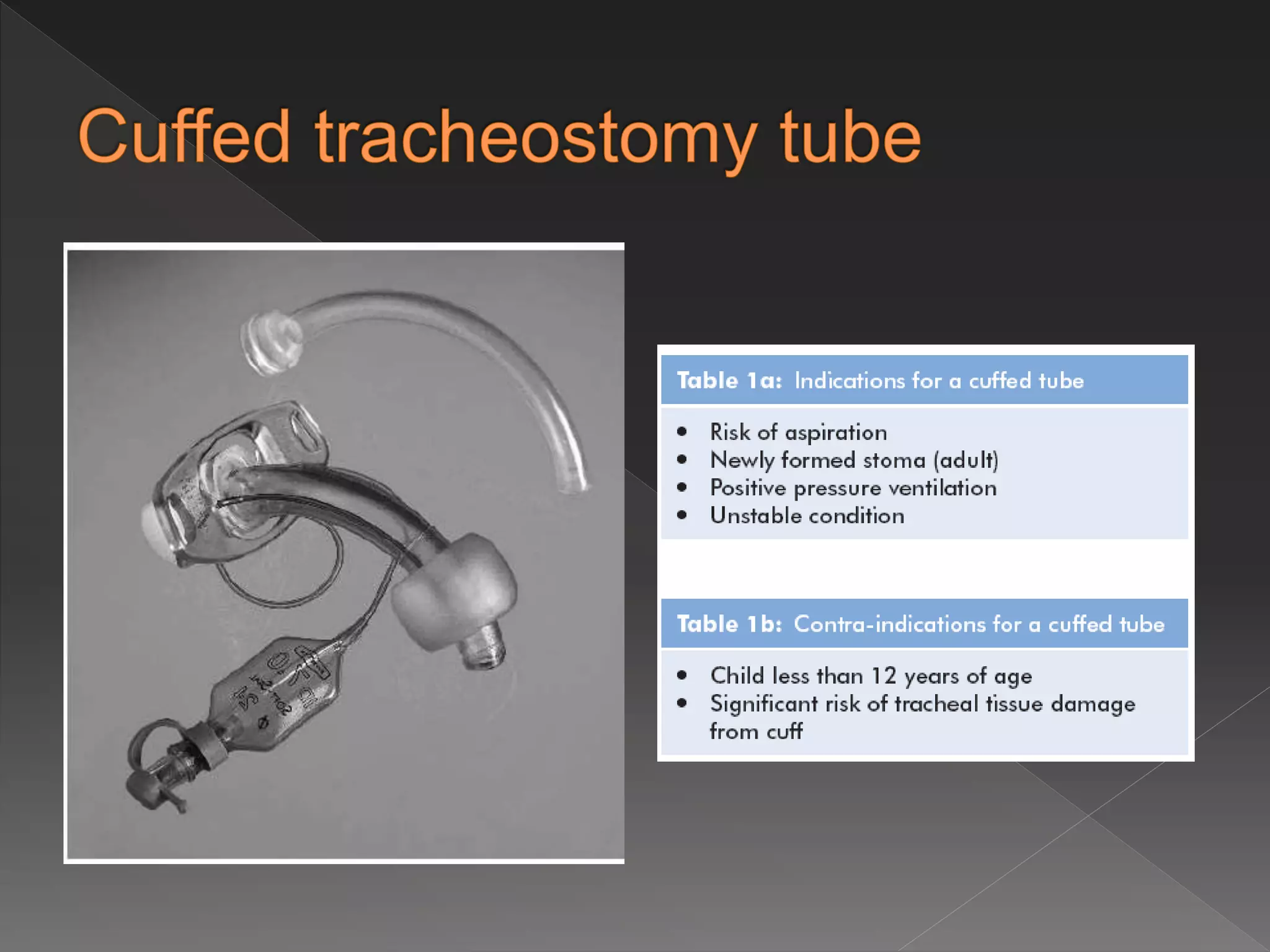
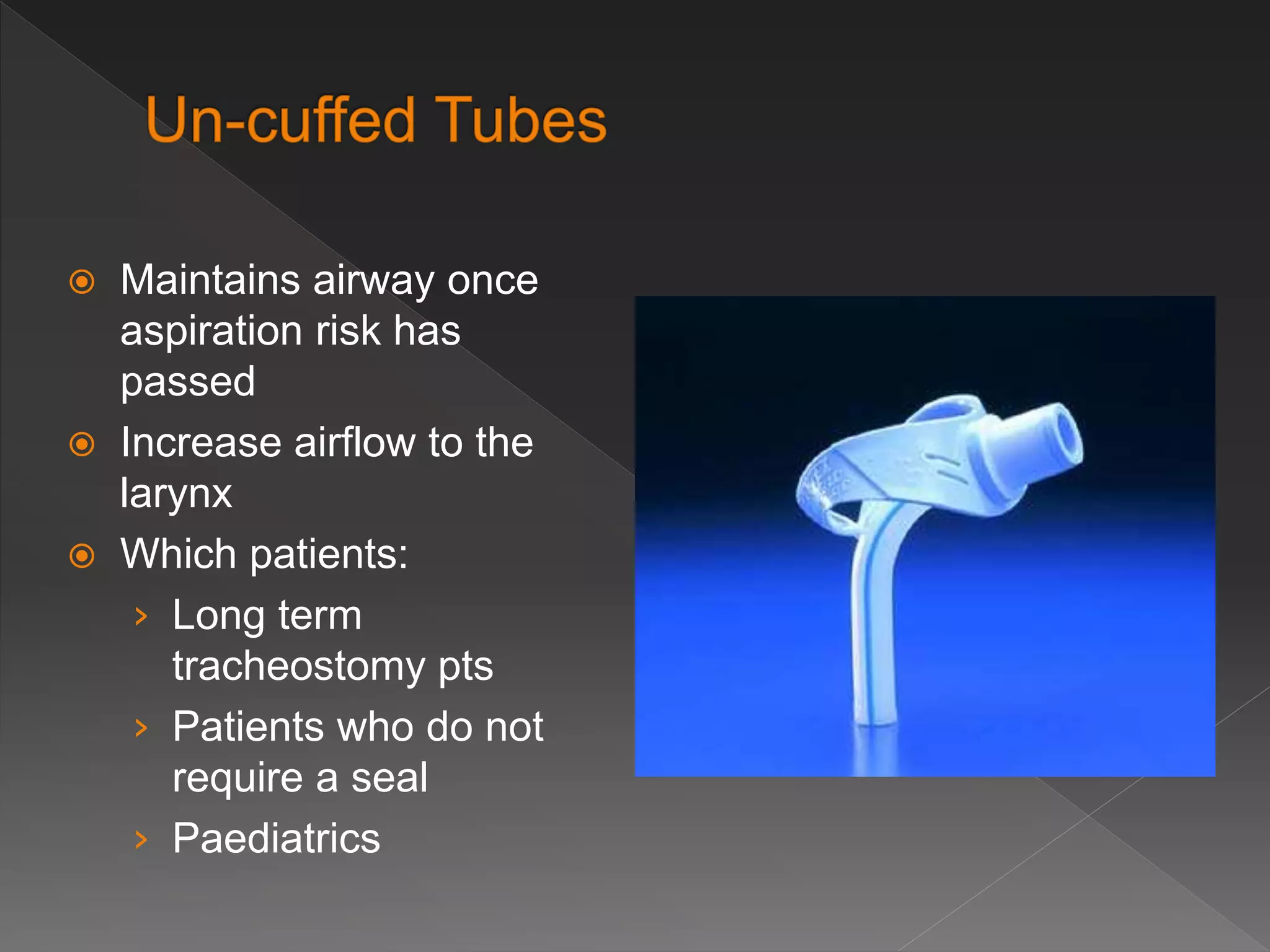
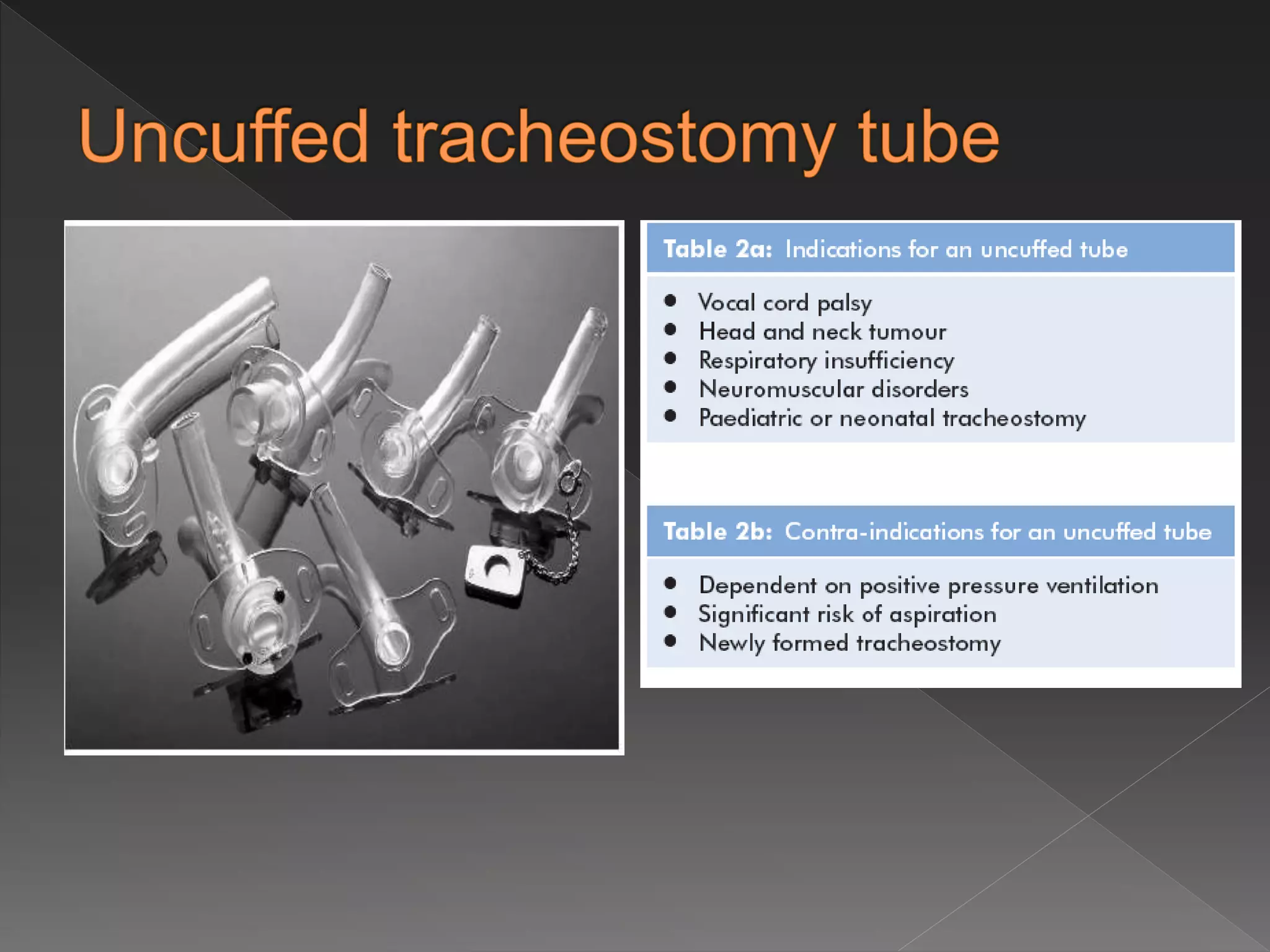



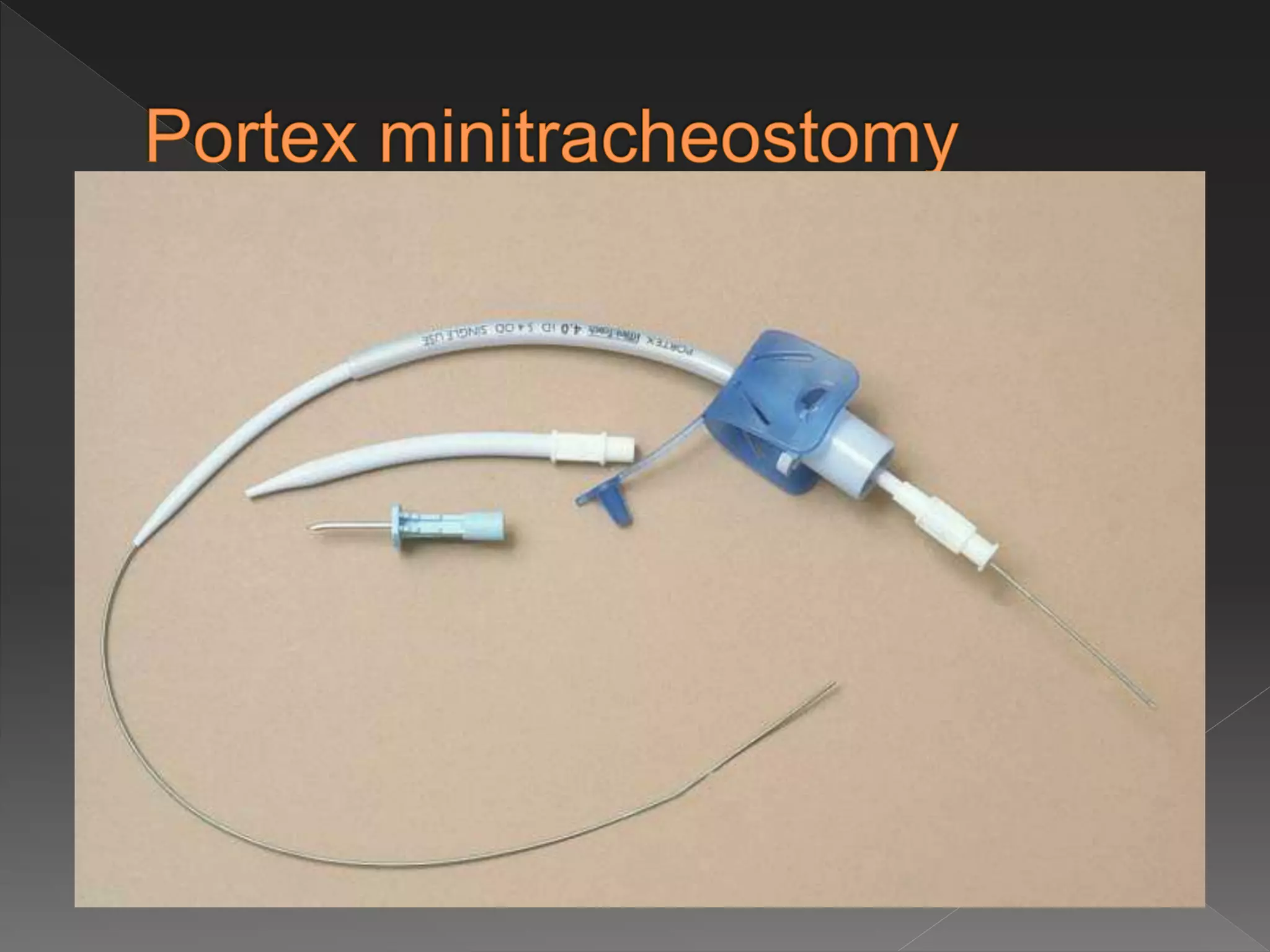





This document discusses tracheostomy, including its definition, indications, procedures, types of tubes, care, and complications. A tracheostomy is a surgical opening into the trachea to allow direct access to the breathing tube. It may be performed to protect the airway, treat respiratory failure or retain secretions. The procedure involves making an incision in the neck and inserting a tracheostomy tube. Tube types include cuffed, uncuffed, and fenestrated. Ongoing care and monitoring for complications is important.























































































