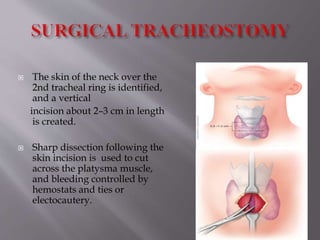
Tracheostomy is a surgical procedure that creates an opening in the trachea to allow direct access to the breathing tube. It is one of the oldest surgical procedures, dating back to the 15th century. Tracheostomies can be temporary or permanent depending on the clinical situation and underlying condition. Potential complications include bleeding, infection, and damage to nearby structures like the thyroid cartilage. Care after tracheostomy involves dressing changes, tube changes or decannulation as appropriate for the patient's recovery.