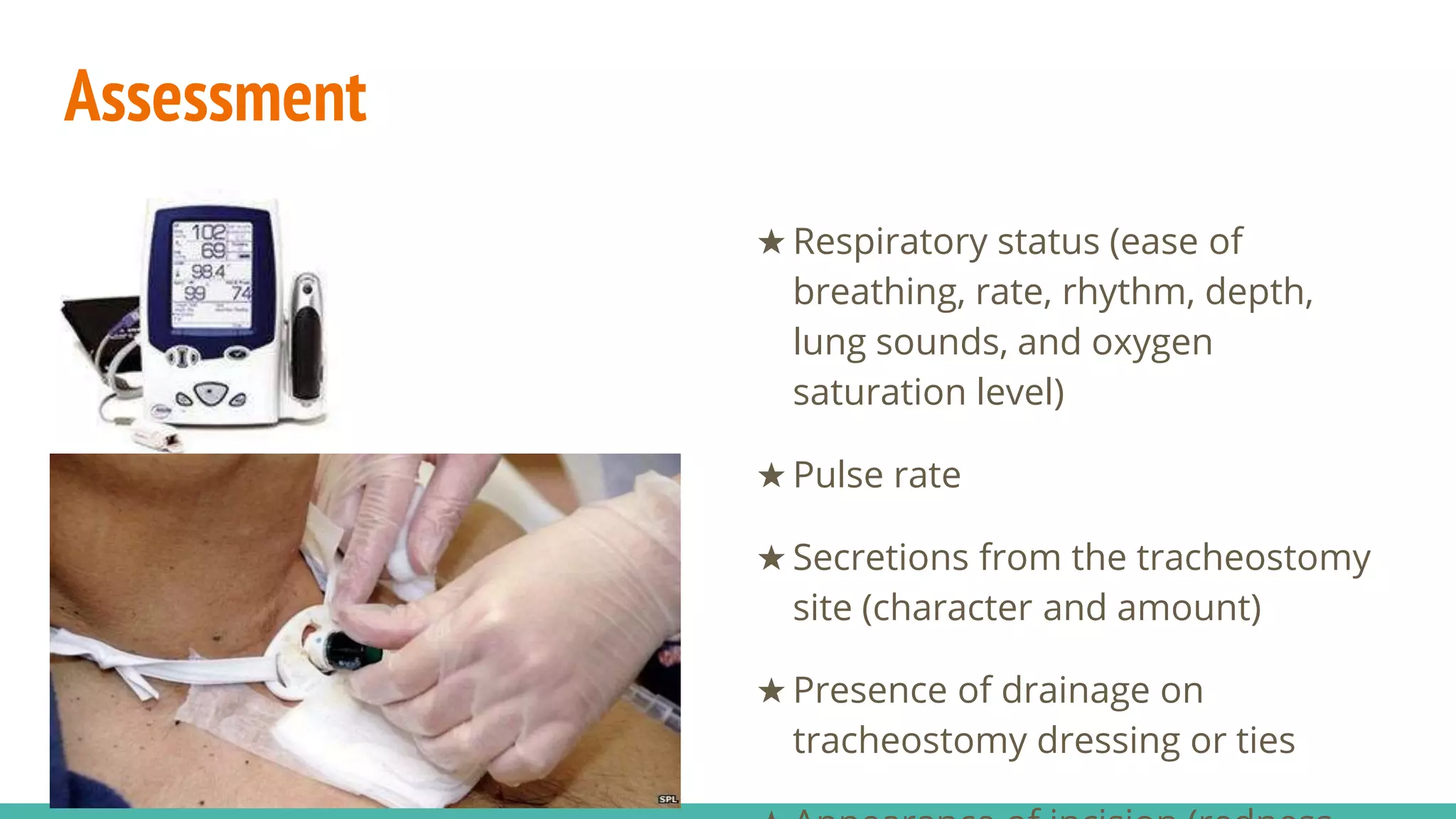
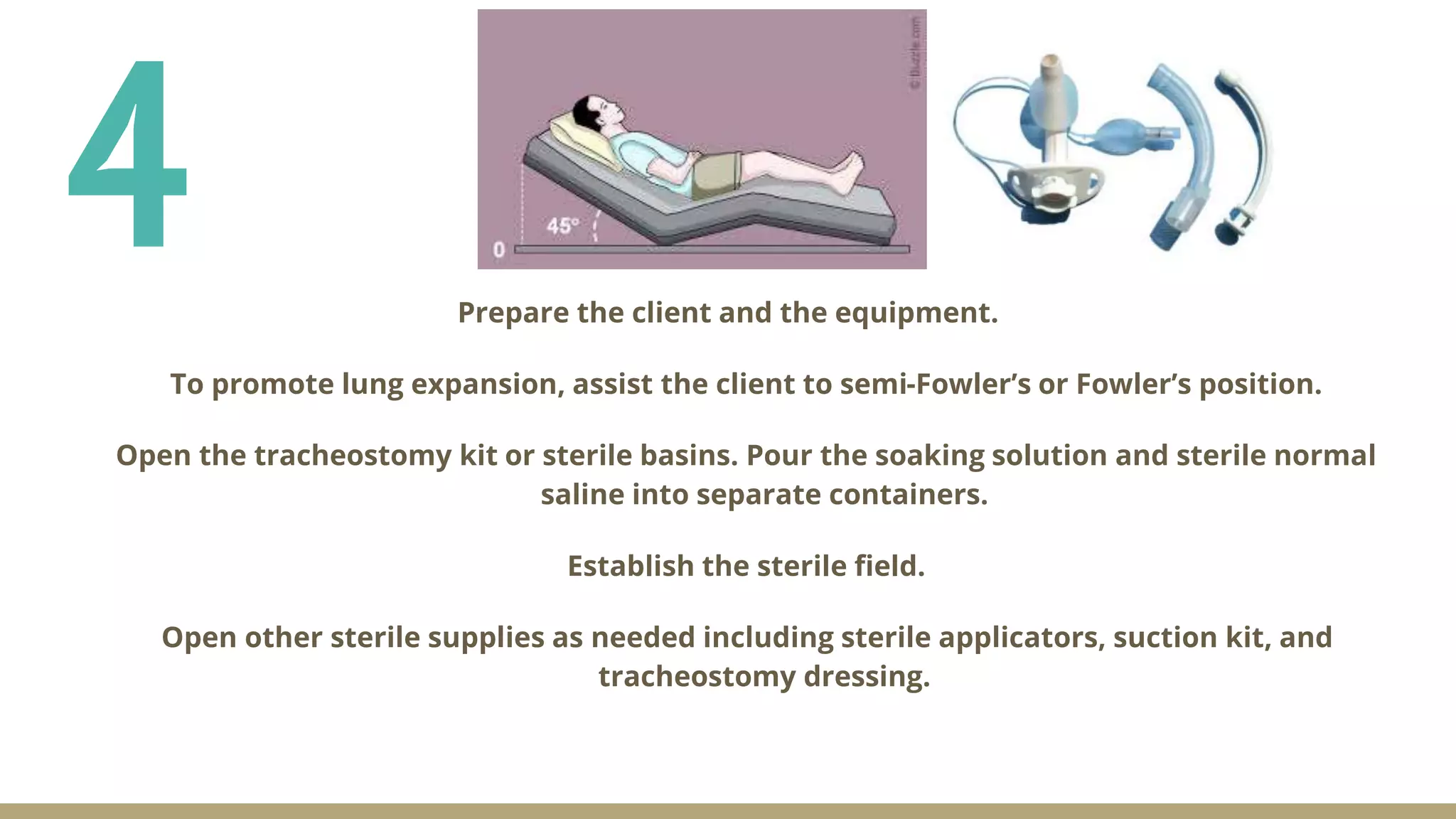
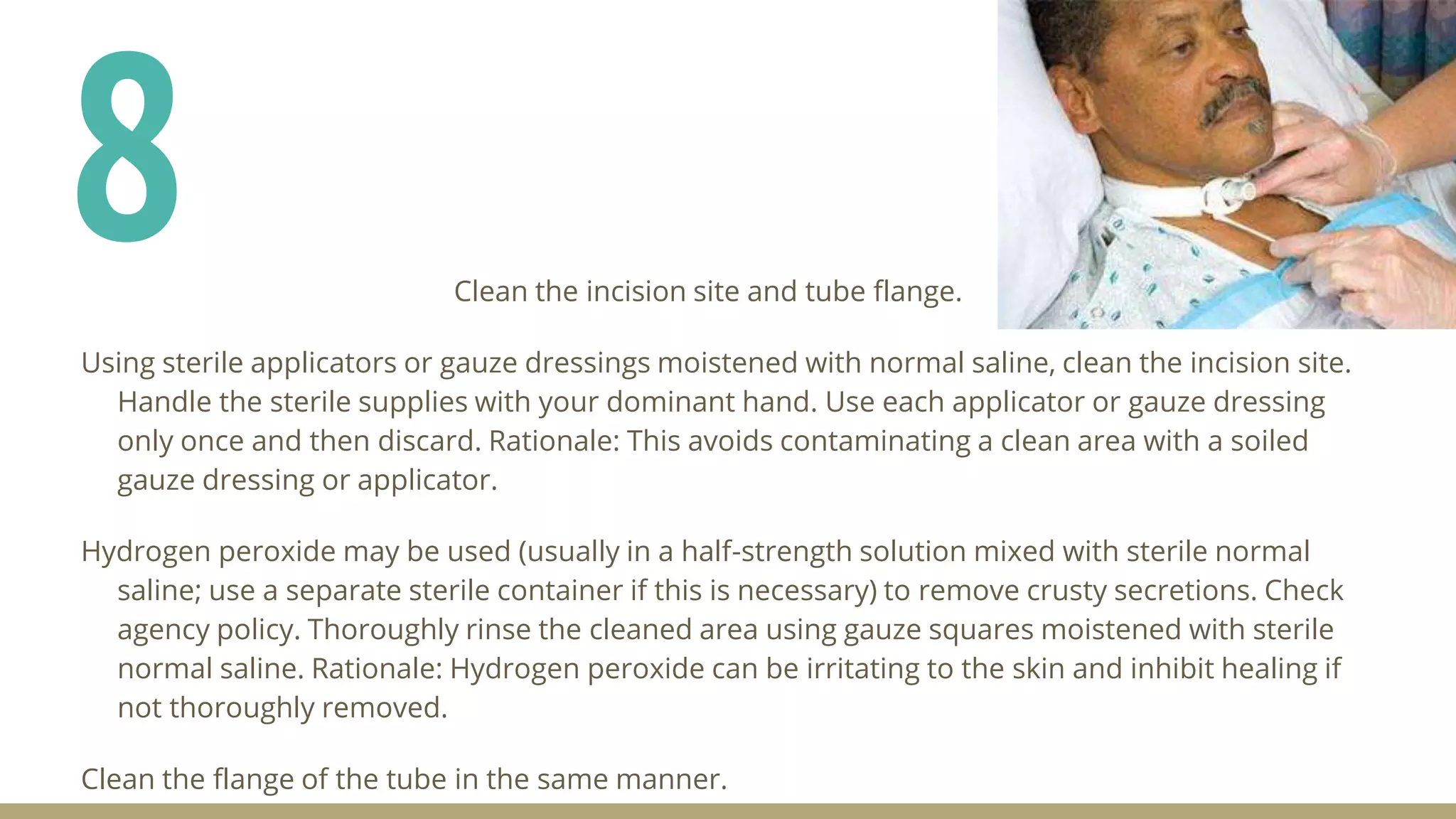
This document provides information on tracheostomy care and management. It defines key terms, outlines the indications for tracheostomy placement, potential complications, proper placement according to anatomy, and the steps for tracheostomy care and management. The goal of tracheostomy care is to maintain airway patency, cleanliness, comfort, and prevent displacement. It describes assessing the patient's respiratory status, secretions, and dressing before performing tracheostomy tube suctioning, cleaning, and dressing changes with the aim of removing secretions and maintaining a clean tracheostomy site.