Downloaded 20 times

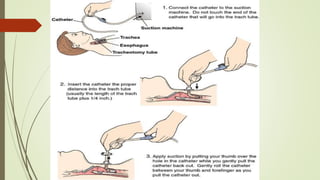

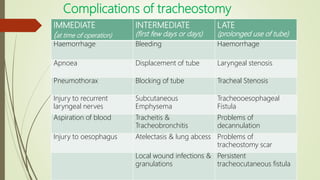


A tracheostomy is a surgically created opening in the trachea to allow for an alternative airway. It has several functions including improving breathing, protecting the airways from aspiration, allowing for suctioning of secretions, and enabling positive pressure ventilation. Tracheostomies can be emergency procedures for acute airway obstruction or elective for longer term issues. The procedure involves making an incision in the neck, separating tissues and strap muscles, opening the trachea, and inserting a tracheostomy tube. Post-operative care focuses on suctioning, tube care, and prevention of complications like infection, bleeding, or stenosis. Tracheostomies may be temporary or permanent depending on the underlying condition.















![Thyroid ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidpptautosaved-170310134424-thumbnail.jpg?width=640&height=640&fit=bounds)