Downloaded 689 times
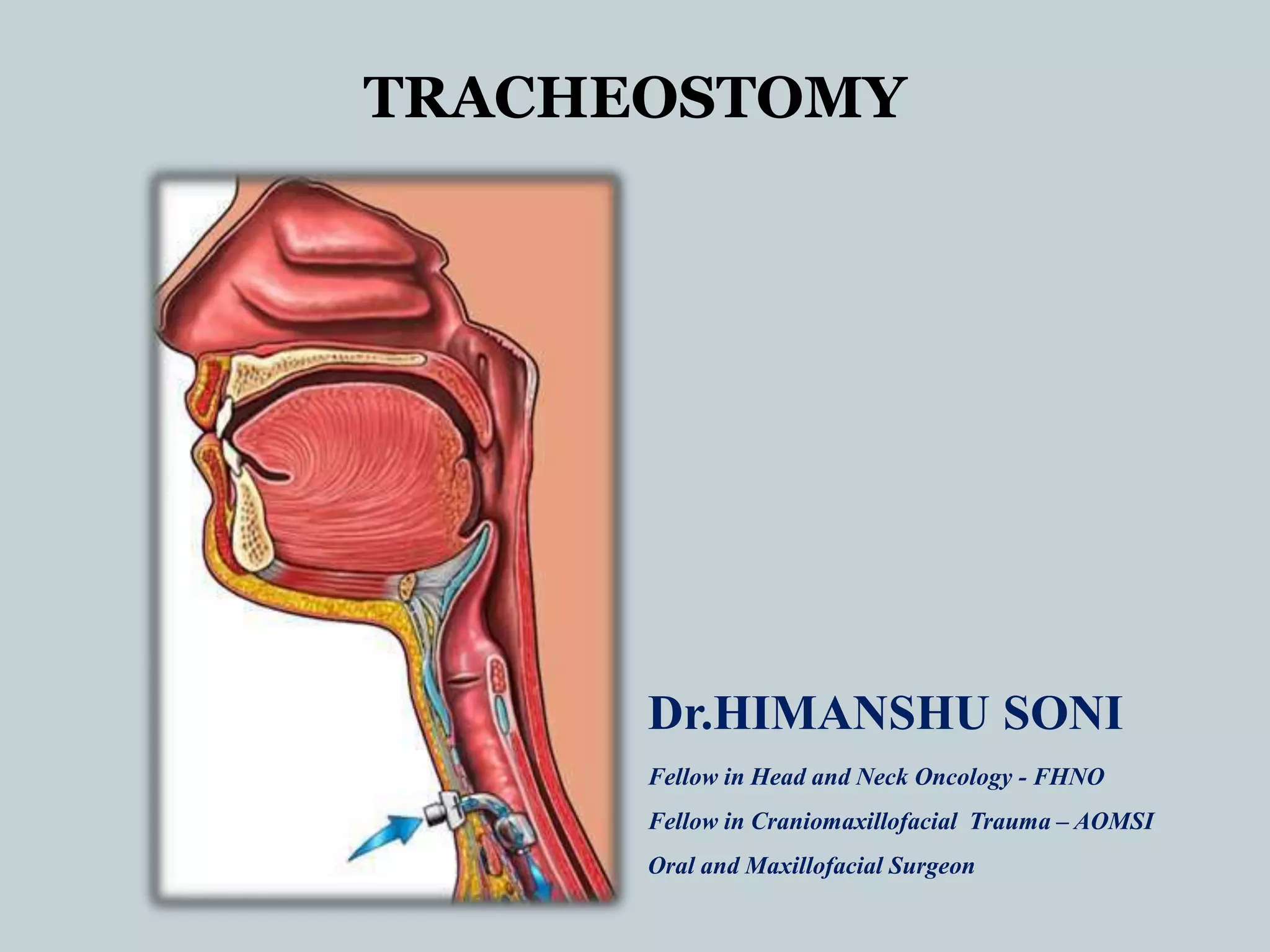
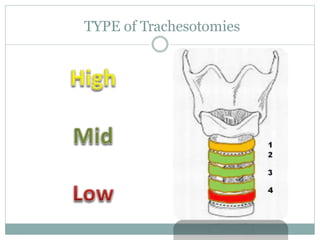
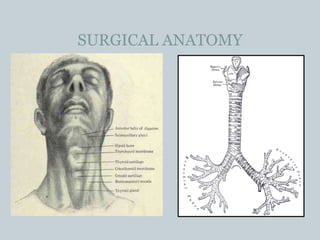
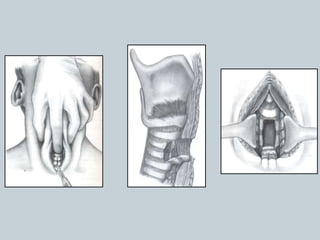
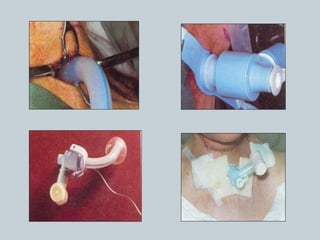
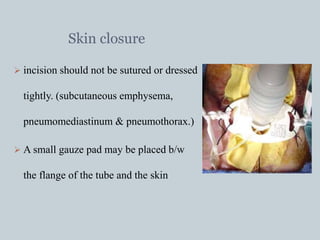



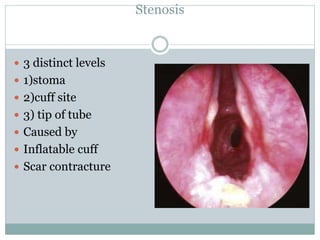
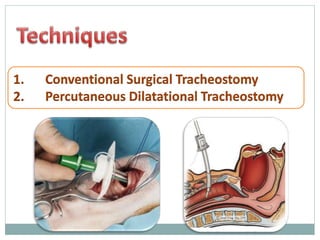
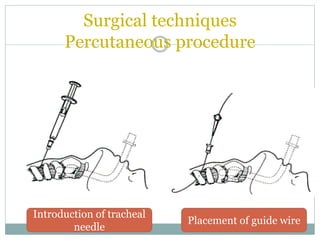
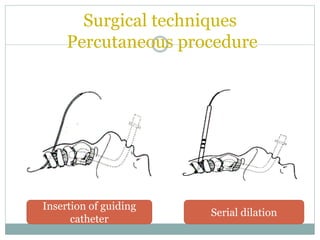



The document provides a comprehensive overview of tracheostomy, including its history, indications, contraindications, surgical techniques, and postoperative care. It discusses the anatomy involved, types of tracheostomy, and complications associated with the procedure. Additionally, guidelines for tracheostomy care and management, especially in pediatric patients, are highlighted, focusing on proper techniques and potential complications.

















































































