Downloaded 29 times

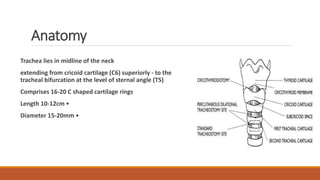






Tracheostomy is a surgical procedure to create an opening into the trachea through the neck. It is used to relieve upper airway obstruction or to facilitate pulmonary toilet. There are different types including emergency, elective, percutaneous dilatational and mini tracheostomy. Complications can occur immediately during the procedure like hemorrhage or apnea, or later from issues like stenosis, infection or tracheoesophageal fistula from prolonged intubation. Careful technique and management of risks are important when performing this procedure to treat upper airway conditions.



































































