Downloaded 2,578 times




































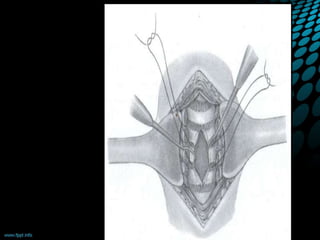































The document discusses tracheostomy, including its history, definitions, indications, types, procedures, complications, and care. Some key points: - Tracheostomy can be traced back to 3600 BC in Egypt and was standardized in technique in the 1920s. Modern percutaneous tracheostomy developed in 1969. - It involves creating a stoma in the trachea that allows for insertion of a tracheostomy tube to bypass upper airway obstruction and facilitate pulmonary ventilation and toilet. - Surgical procedures include open tracheostomy and percutaneous tracheostomy. Complications include bleeding, injury to nearby structures, and long term issues like stenosis. - Ongoing care involves tube maintenance,























































































