Downloaded 37 times


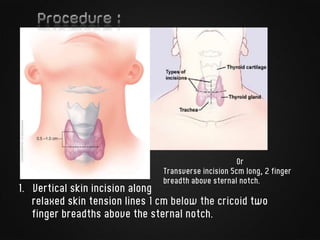
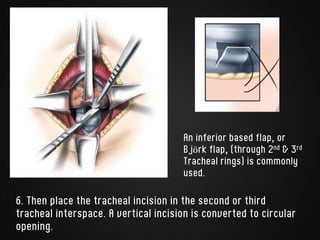
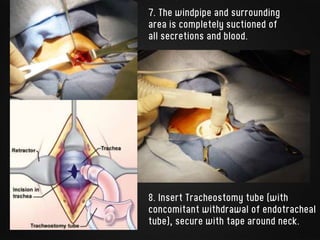



The document summarizes tracheostomy and the tracheostomy procedure. Tracheostomy creates an artificial opening into the trachea. The procedure was first described in the 12th century and the currently used technique was developed by Dr. Chevalier Jackson in the 20th century. The procedure involves making a vertical or transverse incision in the neck, dividing strap muscles, incising the trachea to form an opening, inserting a tracheostomy tube, and securing it. Tracheostomy can be performed as an emergency, electively, or permanently depending on the clinical scenario and patient's condition.












































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





