Downloaded 982 times







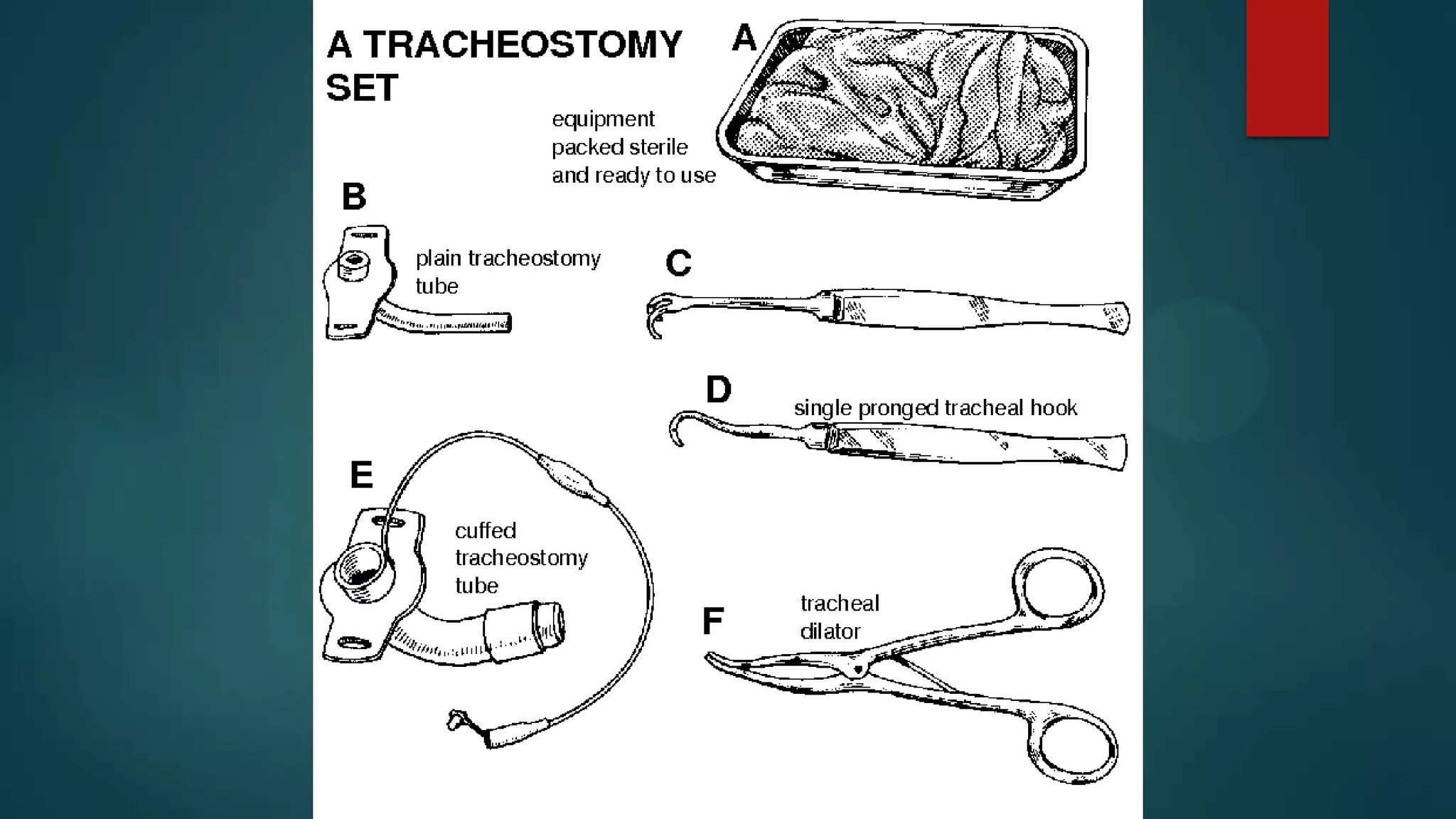






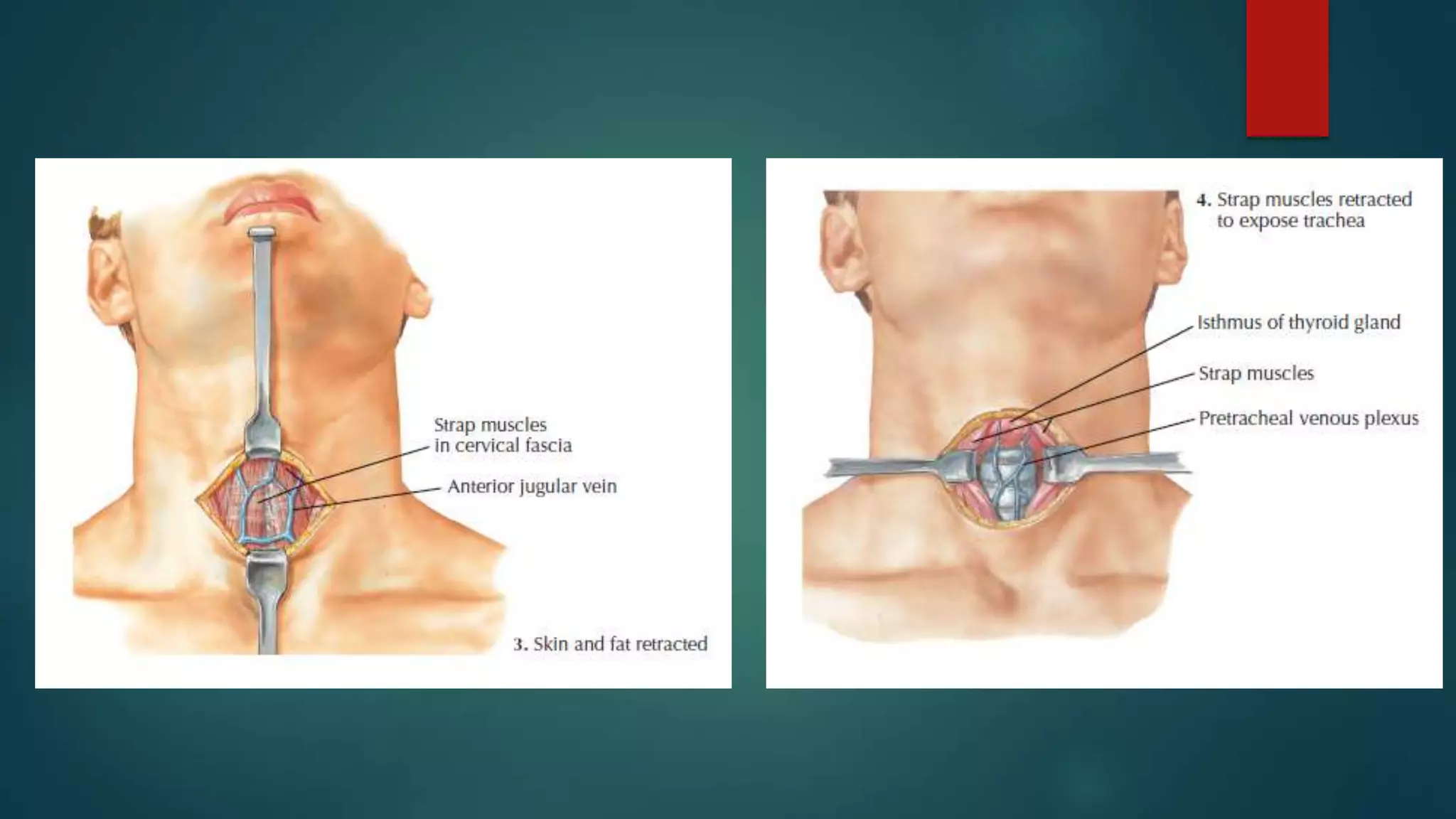








The document provides an overview of tracheostomy, including its definition as a surgical procedure to bypass the airway during upper airway obstruction. It outlines indications and contraindications, the necessary surgical anatomy, procedural steps, and potential complications associated with the operation. Additionally, it describes pre-operative preparations, types of tracheostomy tubes, and post-operative management practices.

































































































