CONTENTS
• Definition
• History
•Brief anatomy of larynx &
trachea
• Types of tracheostomy
• Indications of tracheostomy
• Preoperative check list
• Cricothyroidotomy
• Tracheostomy – conventional
technique
• Paediatric tracheostomy
• Percutaneous procedure
• Mini tracheostomy
• Postoperative management
• Complications
• Decannulation
• Types of tracheostomy tubes
3.
DEFINITION
• TRACHEOTOMY (tomos =to cut ) – HIESTER 1718
surgical procedure in which an opening is made in the anterior wall
of trachea to establish airway often temporary and reversible.
• TRACHEOSTOMY (stoma =mouth) – NEGUS 1938
surgical creation of an opening into trachea through the neck with
the trachea being brought into continuity with the skin most
often ,not always permanent
4.
HISTORY
• 2000 BC– 1st
known reference
• 400 BC - Hippocrates condemned tracheostomy , citing threat to
carotid arteries.
• Hierronymus, Fabricus and Habicot provided the first technical
description of surgical procedure
• 1546 – first successful tracheostomy Antonius Mvsa Brasavola
5.
• 1921- ChevalierJackson defined and refined surgical airway
management technique.
• 1955- percutaneous tracheostomy was described by Shelden
• 1969- Toy and Weinstein described a percutaneous
tracheostomy using the guide wire approach of Seldinger.
• 1985- Ciaglia et al described percutaneous dilation
tracheostomy.
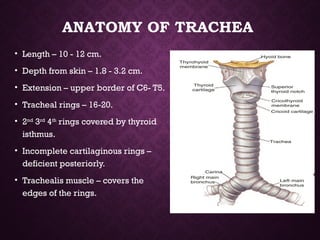
ANATOMY OF TRACHEA
•Length – 10 - 12 cm.
• Depth from skin – 1.8 - 3.2 cm.
• Extension – upper border of C6- T5.
• Tracheal rings – 16-20.
• 2nd
3rd
4th
rings covered by thyroid
isthmus.
• Incomplete cartilaginous rings –
deficient posteriorly.
• Trachealis muscle – covers the
edges of the rings.
8.
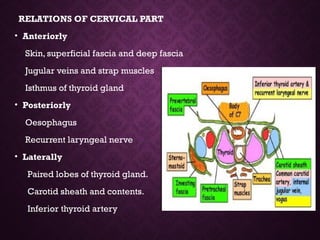
RELATIONS OF CERVICALPART
• Anteriorly
Skin, superficial fascia and deep fascia
Jugular veins and strap muscles
Isthmus of thyroid gland
• Posteriorly
Oesophagus
Recurrent laryngeal nerve
• Laterally
Paired lobes of thyroid gland.
Carotid sheath and contents.
Inferior thyroid artery
9.
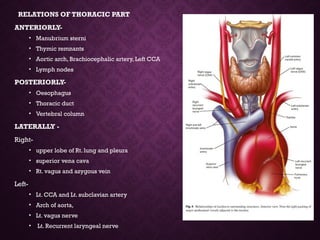
RELATIONS OF THORACICPART
ANTERIORLY-
• Manubrium sterni
• Thymic remnants
• Aortic arch, Brachiocephalic artery, Left CCA
• Lymph nodes
POSTERIORLY-
• Oesophagus
• Thoracic duct
• Vertebral column
LATERALLY -
Right-
• upper lobe of Rt. lung and pleura
• superior vena cava
• Rt. vagus and azygous vein
Left-
• Lt. CCA and Lt. subclavian artery
• Arch of aorta,
• Lt. vagus nerve
• Lt. Recurrent laryngeal nerve
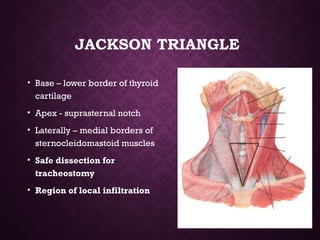
JACKSON TRIANGLE
• Base– lower border of thyroid
cartilage
• Apex - suprasternal notch
• Laterally – medial borders of
sternocleidomastoid muscles
• Safe dissection for
tracheostomy
• Region of local infiltration
13.
FUNCTIONS OF TRACHEOSTOMY
1.Alternative pathway for breathing– circumvents any obstruction in the upper
airway from lips to the tracheostome.
2. Improves alveolar ventilation-- In cases of respiratory insufficiency, alveolar
ventilation is improved by–
• Decreasing the dead space by 30-50% (normal dead space is 150 ml)
• Reducing the resistance to airflow.
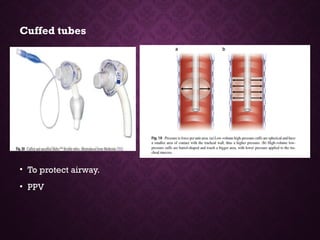
3. Protects the airways. By using cuffed tube, tracheobronchial tree is protected
against aspiration of:
• Pharyngeal secretions, as in case of bulbar paralysis or coma.
• Blood, as in haemorrhage from pharynx, larynx or maxillofacial injuries
• With tracheostomy, pharynx and larynx can also be packed to control
bleeding.
14.
4. Permits removalof tracheobronchial secretions---
• When patient is unable to cough as in coma , head injuries,
respiratory paralysis
• when cough is painful , as in chest injuries or upper abdominal
operations
• the tracheobronchial airway can be kept clean of secretions by
repeated suction through the tracheostomy, thus avoiding need
for repeated bronchoscopy or intubation which is not only
traumatic but requires expertise .
5. Intermittent positive pressure respiration (IPPR)--- If IPPR is required
beyond 72 hours, tracheostomy is superior to intubation.
6.To administer anaesthesia. In cases where endotracheal intubation is
difficult or impossible as in laryngopharyngeal growths or trismus.
15.
TYPES OF TRACHEOSTOMY
•Emergency tracheostomy
• Elective tracheostomy
• Permanent tracheostomy
• Percutaneous dilatational tracheostomy
• Mini tracheostomy /Cricothyroidotomy
16.
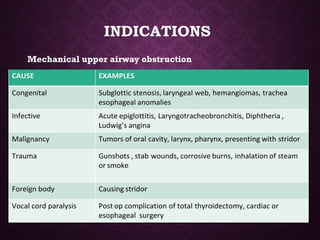
EMERGENCY TRACHEOSTOMY
• Itis employed when airway obstruction is complete or almost
complete and
• There is an urgent need to establish the airway.
• Intubation or laryngotomy are either not possible or feasible in
such cases.
17.
ELECTIVE TRACHEOSTOMY
• Thisis a planned procedure. Almost all operative surgical facilities
available, endotracheal tube can be put and local or general
anaesthesia can be given.
• It is of two types:
• A)Therapeutic: to relieve respiratory obstruction, remove
tracheobronchial secretions, or give assisted ventilation.
• B)Prophylactic: to guard against anticipated respiratory
obstruction or aspiration of blood or pharyngeal secretions such as
in extensive surgery of tongue, floor of mouth, mandibular
resection or laryngofissure.
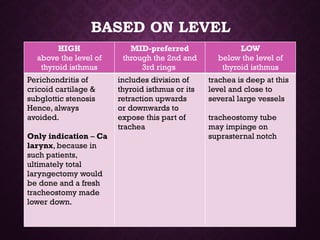
BASED ON LEVEL
HIGH
abovethe level of
thyroid isthmus
MID-preferred
through the 2nd and
3rd rings
LOW
below the level of
thyroid isthmus
Perichondritis of
cricoid cartilage &
subglottic stenosis
Hence, always
avoided.
Only indication – Ca
larynx, because in
such patients,
ultimately total
laryngectomy would
be done and a fresh
tracheostomy made
lower down.
includes division of
thyroid isthmus or its
retraction upwards
or downwards to
expose this part of
trachea
trachea is deep at this
level and close to
several large vessels
tracheostomy tube
may impinge on
suprasternal notch
Protection of lowerairway from aspiration
• A cuffed tube will prevent inhalation of fluids and the tube allows
easy access to trachea and the bronchi for suction.
• Neurological disease --GBS, motor neuron disease, bulbar
poliomyelitis, multiple sclerosis, tetanus, brain stem stroke and
bulbar palsy.
• Coma (GCS<8)- protective reflexes lost –risk of aspiration– head
injury, poisoning and brain tumours.
• Trauma – severe facial fractures-- result in aspiration of blood from
the upper airways.
22.
Respiratory failure
• Tracheostomyreduces dead space by 50%- less effort in
breathing and increased alveolar ventilation.
• easy access to the respiratory tree for suctioning and removal of
bronchial secretions.
• Examples:-
• Pulmonary diseases (exacerbation of chronic bronchitis and
emphysema, severe asthma, severe pneumonia).
• Neurological diseases(multiple sclerosis, motor neuron disease).
• Severe chest injury( flail chest)
23.
• Retention ofbronchial secretions
• chronic pulmonary disease
• acute respiratory infection
• decreased level of consciousness
• trauma to the thoracic cage or musculature with ineffective
cough and retention of secretions.
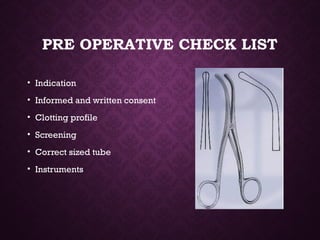
PRE OPERATIVE CHECKLIST
• Indication
• Informed and written consent
• Clotting profile
• Screening
• Correct sized tube
• Instruments
27.
TYPES OF TRACHEOSTOMY
TUBES
•Plastic and metal
• Cuffed and uncuffed
• Fenestrated and unfenestrated
• Single and double lumen
28.
Metal tubes
• madeof silver or stainless steel.
• Advantages -- endurable, inert, and resistant to biofilm formation;
they limit bacterial growth; can be easily sanitized and sterilized ,
more cost effective for long-term use
• Disadvantages-- inelastic, do not have a cuff or a connector for
mechanical ventilation, can harm the trachea by heat or cold injury,
hence not suitable for patients on radiation therapy whose radiation
field is near the device.
• available from size 00 to size 12.
30.
PLASTIC TUBES
• Madeup of polyvinyl chloride or silicone
• semiflexible( adapts to the patient’s anatomy, normally has a right angle and a
longer cannula) or rigid( does not collapse or deflect, does not have a right
angle, and is usually used for neck swelling, but it is not suitable for patients
with thick necks, since its main shaft is short)
• insertion is aided by an obturator.
• Can be made with cuff
• It has connector to anaesthetic machine and ventilator
• Cause less mechanical damage to trachea.
• PVC adjusts to the patient’s temperature and anatomy
• Silicone is soft, does not retain heat or cold, resistant to colonization and biofilm,
and can be sterilized
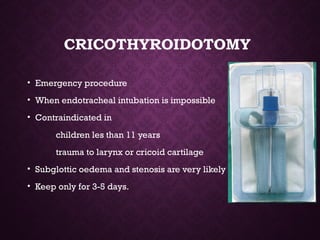
CRICOTHYROIDOTOMY
• Emergency procedure
•When endotracheal intubation is impossible
• Contraindicated in
children les than 11 years
trauma to larynx or cricoid cartilage
• Subglottic oedema and stenosis are very likely
• Keep only for 3-5 days.
LAYERS OF DISSECTION
•Skin
• Adipose tissue
• Platysma
• Anterior jugular veins and anastamosis between them
• Strap muscles
• Thyroid isthmus
• Trachea
42.
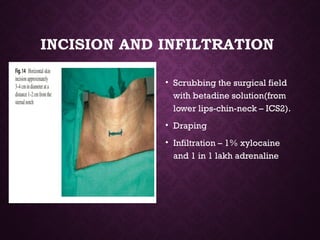
INCISION AND INFILTRATION
•Scrubbing the surgical field
with betadine solution(from
lower lips-chin-neck – ICS2).
• Draping
• Infiltration – 1% xylocaine
and 1 in 1 lakh adrenaline
43.
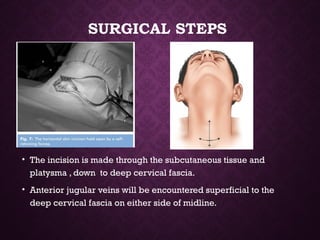
SURGICAL STEPS
• Theincision is made through the subcutaneous tissue and
platysma , down to deep cervical fascia.
• Anterior jugular veins will be encountered superficial to the
deep cervical fascia on either side of midline.
44.
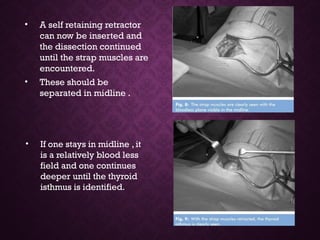
• A selfretaining retractor
can now be inserted and
the dissection continued
until the strap muscles are
encountered.
• These should be
separated in midline .
• If one stays in midline , it
is a relatively blood less
field and one continues
deeper until the thyroid
isthmus is identified.
45.
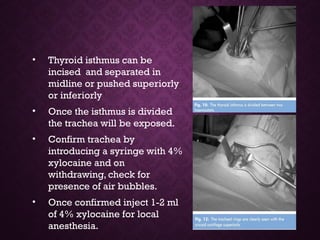
• Thyroid isthmuscan be
incised and separated in
midline or pushed superiorly
or inferiorly
• Once the isthmus is divided
the trachea will be exposed.
• Confirm trachea by
introducing a syringe with 4%
xylocaine and on
withdrawing, check for
presence of air bubbles.
• Once confirmed inject 1-2 ml
of 4% xylocaine for local
anesthesia.
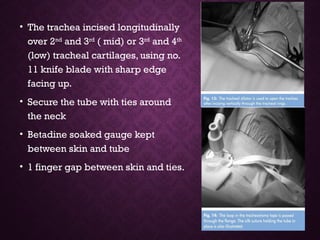
• The tracheaincised longitudinally
over 2nd
and 3rd
( mid) or 3rd
and 4th
(low) tracheal cartilages, using no.
11 knife blade with sharp edge
facing up.
• Secure the tube with ties around
the neck
• Betadine soaked gauge kept
between skin and tube
• 1 finger gap between skin and ties.
48.
WHEN PERFORMING INAN
INTUBATED PATIENT
• Before making the incision in the trachea – withdraw the
endotracheal tube.
• Should not puncture the cuff of the endotracheal tube.
• Tube pushed further down the trachea towards the carina
before making the hole. Once the trachea is incised the tube is
withdrawn under direct vision until the tip is just above the
incision.
• In vertical incision- tracheal dilators will be needed.
49.
WHEN CAN WECHANGE ?
• The tube should only be changed once a tract has formed
between the trachea and the skin.
• This only occurs after 48 -72 h, so the tube should not be
replaced until at least 3 days.
50.
BJORK FLAP
• Inferiorlybased anterior tracheal wall flap.
• Sutured onto the skin to exteriorize trachea.
• Disadvantages :
suture break- difficult for reinsertion of tube.
difficult spontaneous closure of stoma.
tracheal stenosis.
ANATOMY IN CHILDREN
•In children, the neck and trachea are smaller.
• The trachea is more elastic and extensible -- properties that are
reduced with the aging calcification process.
• also deeper and more mobile than in adults
• Pulmonary reserve is also reduced in cases of apnea, for example.
In this way, accidental displacement of the cannula is a high-risk
maneuver.
• Fixing the cannula to the skin through single stitches is an option to
prevent this accidental removal.
53.
• Better doneunder general anaesthesia
• Neck should not be over extended
• Vertical incision between 2nd
and 3rd
tracheal
ring.
• Removal of subcutaneous fat & maturation sutures
• No excision of anterior wall of trachea.
• Margins of tracheal incision sutured to skin.
55.
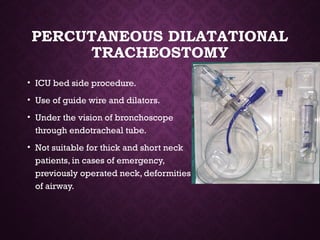
PERCUTANEOUS DILATATIONAL
TRACHEOSTOMY
• ICUbed side procedure.
• Use of guide wire and dilators.
• Under the vision of bronchoscope
through endotracheal tube.
• Not suitable for thick and short neck
patients, in cases of emergency,
previously operated neck, deformities
of airway.
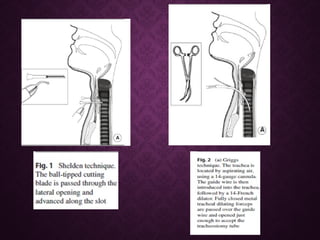
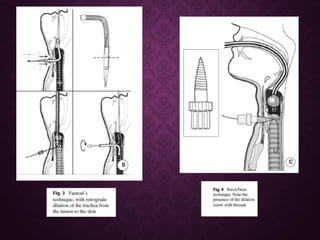
PERCUTANEOUS DILATATIONAL
TRACHEOSTOMY
variants ---
•Using a wire guided sharp forceps ( Griggs technique)
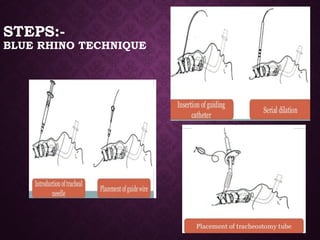
• Using a single tapered dilator ( Blue Rhino)
• Passing the dilator from inside the trachea to the outside
(Fantoni’s technique)
• Using a screw like device to open the trachea wall (Perc Twiat).
60.
MINI TRACHEOSTOMY
• Verticalstab incision made through the cricothyroid
membrane under local anaesthesia allows the insertion of a 4
mm cannula to provide ready access and delivery of oxygen.
• Described by Mathews and Hopkinson in 1984
• INDICATIONS :To remove chest secretions
respiratory failure
POST OPERATIVE MANAGEMENT
•X ray soft tissues neck- lateral view
• Analgesics
• Antibiotics
• IV fluid until able to tolerate orally
63.
RISK FACTORS FOR
COMPLICATIONS
•Age: infants and adults over 75
• Obesity
• Smoking
• Poor nutrition
• Recent illness, especially an upper respiratory tract infection
• Alcoholism
• Chronic illness
• Diabetes
64.
COMPLICATIONS
Immediate Intermediate /early
post-operative
Late post- operative
Hemorrhage
Airway fire
Injury to trachea and
larynx
Injury to para tracheal
structures
Air embolism
Apnea
Cardiac arrest
Subcutaneous
emphysema
Pneumothorax/
pneumomediastinum
Tube displacement
Tube blockage
Wound infection
Tracheal necrosis
Secondary haemorrhage
Swallowing problems
Granuloma formation
Tracheo-oesophageal
fistula
Difficult decannulation
Tracheo-cutaneous
fistula
Laryngo-tracheal
stenosis
Tracheostomy
scar/keloid
Foreign body trachea
65.
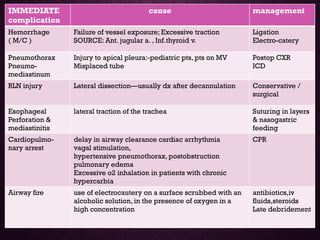
IMMEDIATE
complication
cause management
Hemorrhage
( M/C)
Failure of vessel exposure; Excessive traction
SOURCE: Ant. jugular a. , Inf.thyroid v.
Ligation
Electro-catery
Pneumothorax
Pneumo-
mediastinum
Injury to apical pleura:-pediatric pts, pts on MV
Misplaced tube
Postop CXR
ICD
RLN injury Lateral dissection—usually dx after decannulation Conservative /
surgical
Esophageal
Perforation &
mediastinitis
lateral traction of the trachea Suturing in layers
& nasogastric
feeding
Cardiopulmo-
nary arrest
delay in airway clearance cardiac arrhythmia
vagal stimulation,
hypertensive pneumothorax, postobstruction
pulmonary edema
Excessive o2 inhalation in patients with chronic
hypercarbia
CPR
Airway fire use of electrocautery on a surface scrubbed with an
alcoholic solution, in the presence of oxygen in a
high concentration
antibiotics,iv
fluids,steroids
Late debridement
66.
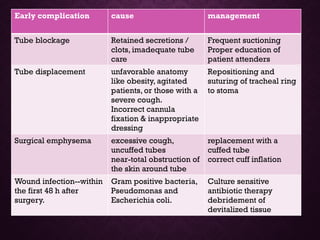
Early complication causemanagement
Tube blockage Retained secretions /
clots, imadequate tube
care
Frequent suctioning
Proper education of
patient attenders
Tube displacement unfavorable anatomy
like obesity, agitated
patients, or those with a
severe cough.
Incorrect cannula
fixation & inappropriate
dressing
Repositioning and
suturing of tracheal ring
to stoma
Surgical emphysema excessive cough,
uncuffed tubes
near-total obstruction of
the skin around tube
replacement with a
cuffed tube
correct cuff inflation
Wound infection--within
the first 48 h after
surgery.
Gram positive bacteria,
Pseudomonas and
Escherichia coli.
Culture sensitive
antibiotic therapy
debridement of
devitalized tissue
67.
Late complication causemanagement
Tracheal stenosis sepsis, stoma infection,
hypotension, elderly pts,
steroids, cannula size,
excessive cannula mobility,
prolonged cannulation,
disproportionate excision of
anterior wall of trachea
CT & tracheoscopy
Laser excision of
granulation tissue
Bronchoscopic
dilatation
Resection and
reanasthmosis
tracheomalacia secondary to chondritis retracheostomy,
stent placement,
tracheal resection
Tracheo-
innominate fistula
fatal
local trauma secondary to
excessive movement of the
tracheal cannula,
hyperinflation of the cuff,
inferior placement of cannula
bleeding prodrome by
tracheostomy, evolving
to massive hemoptysis.
Immediate surgical
exploration to
correct the fistula
Tracheo-
oesophageal fistula
trauma to the posterior wall of
the trachea
Surgical –cervical/
thoracic approach
69.
TRACHEOSTOMY CARE
• Suctioning
regular gentle suctioning
Not aggressive not too much deep
• Skin care
Meticulous wound and stoma care
To prevent irritation and secondary inflammation due to discharge
• Inner tube care
once or more daily removed and cleaned
• Humidification
artificial nose to prevent crusting of secretions
• Tube position
to prevent decubitus of trachea
not to cover with blanket.
70.
TRACHEOSTOMY CARE
Care ofcuff
When to inflate the cuff
• Immediately post operatively – to prevent aspiration of blood or
serous fluid from the wound
• To seal the trachea during mechanical ventilation.
• To prevent aspiration of leakage from tracheo-oesophageal fistula
• To prevent aspiration due to laryngeal incompetence
How to Deflate
• First suction the oropharynx
• Cuff should be deflated at least 5 min every hour.
71.
CHANGING THE
TRACHEOSTOMY TUBE
Indications:soiled ,blocked, cuff rupture
changed to smaller size or another type
Avoid within first week
First tube changed by the surgeon
Difficult cases ( obese, short ,thick neck ) be prepared for
endotracheal intubation
72.
HOME CARE
• Educationand training of the
attendant
• Should have suction catheter
and suction machine
• Educate them when to come
to hospital
• If tube is blocked , advise to
remove inner tube or entire
tracheostomy tube and come
to hospital.
73.
DECANNULATION
• Procedure ofrestoring the physiological pathway of respiration
with withdrawal of tracheostomy tube.
• Should be left in place no longer than necessary
• As soon as the patient condition permits, reduce the size of tube to
avoid physiologic dependence on a large tube.
• Check for adequacy of airway, ability to swallow and handle
secretions for 24 hours and then plug the tube.
• If occlusion tolerated for 24 hours, the tube is removed and
tracheo-cutaneous fistula is taped shut.
75.
DECANNULATION
• Bronchoscopy beforedecannulation in the paediatric patient
• Immediately after decannulation the patient must be closely
observed, and means for re-establishing the airway must be at
hand
• Healing of wound takes place in few days or weeks
• Rarely secondary closure of wound is required.
76.
REFERENCES
1. SCOTT BROWN8TH
EDITION VOLUME 2
2. TRACHEOSTOMY , SPRINGER PUBLICATIONS
3. LOGAN TURNER DISEASES OF EAR, NOSE & THROAT 11TH
EDITION
Thank you …





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
