Download as PDF, PPTX
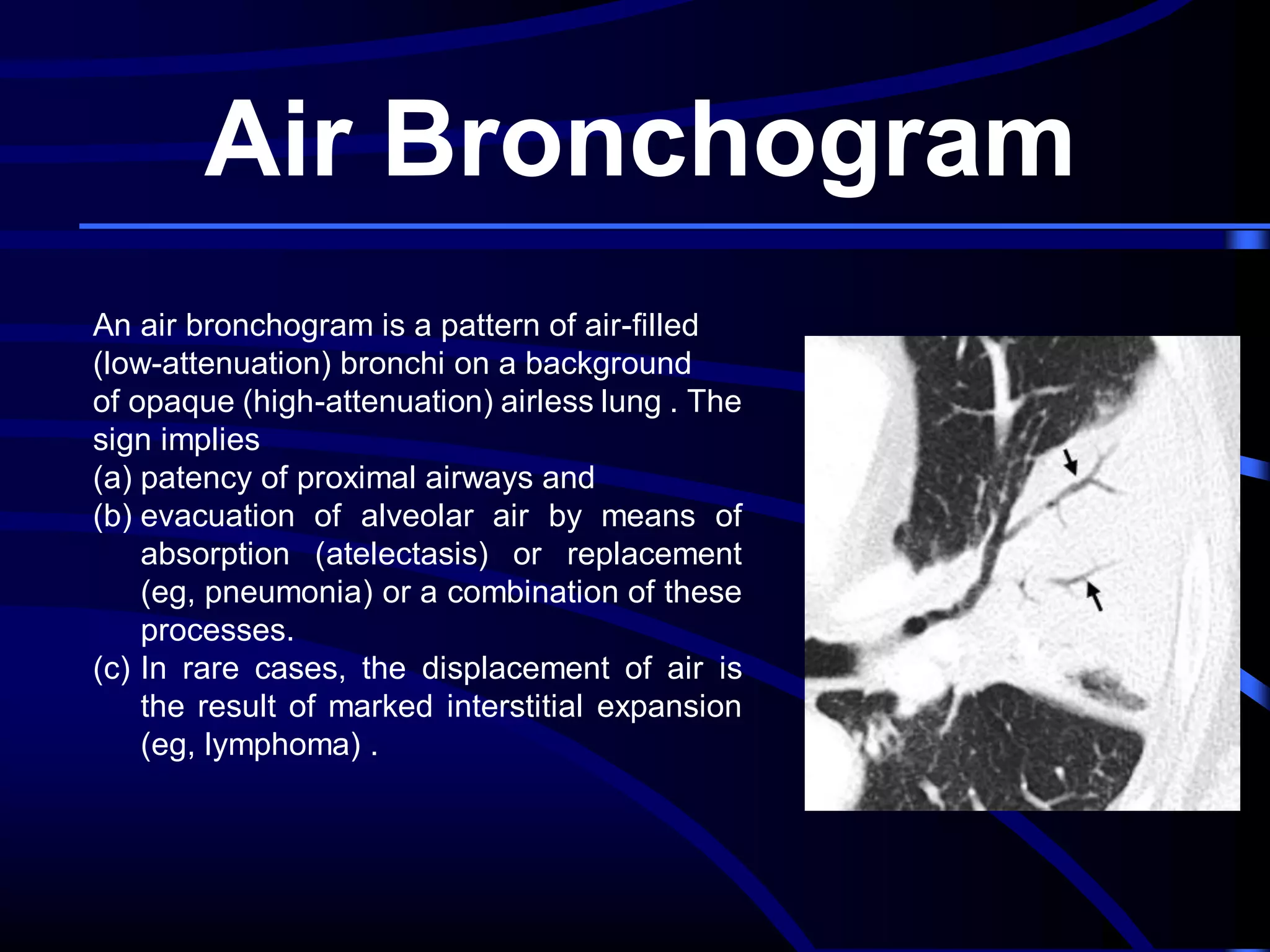

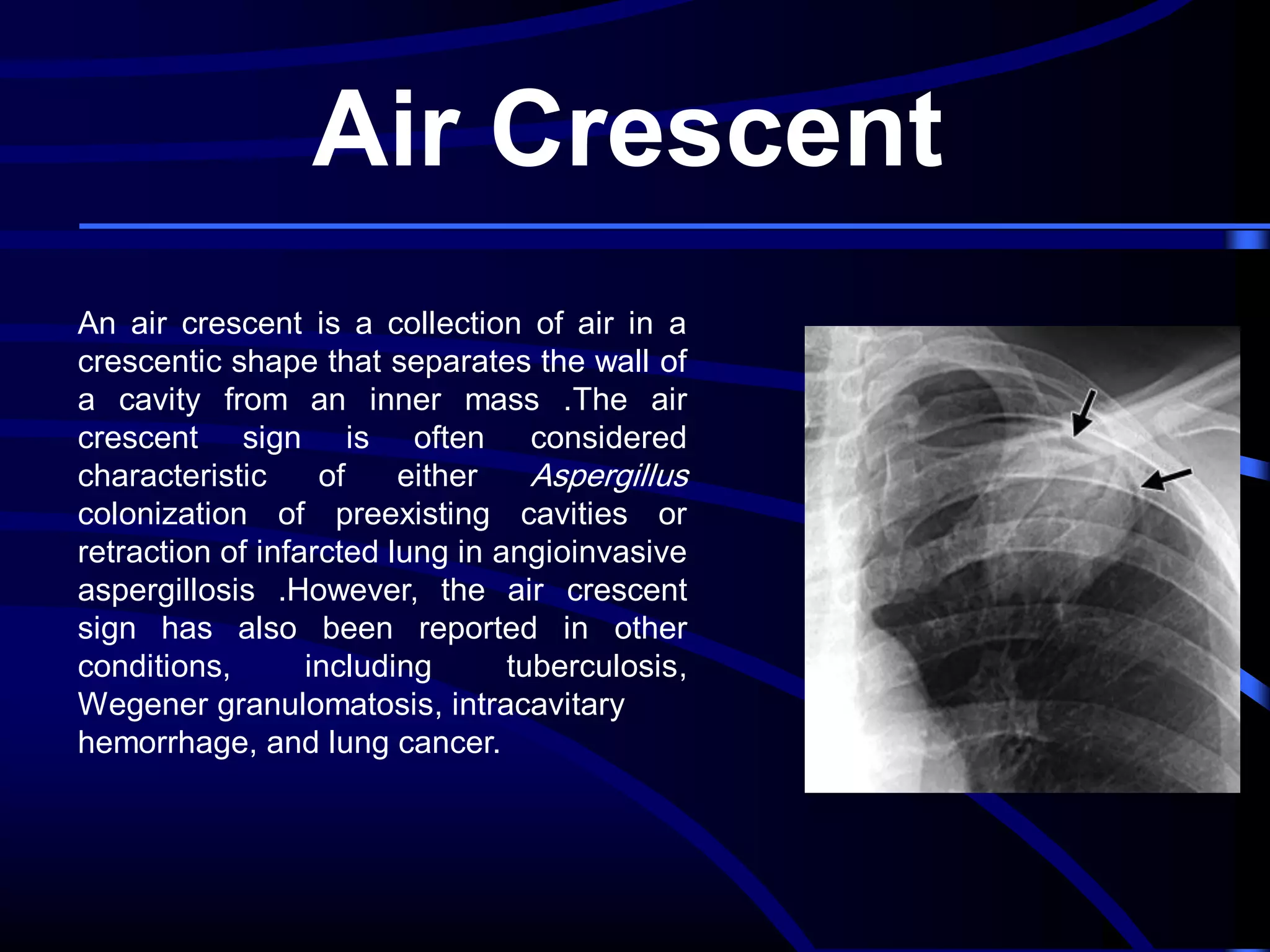
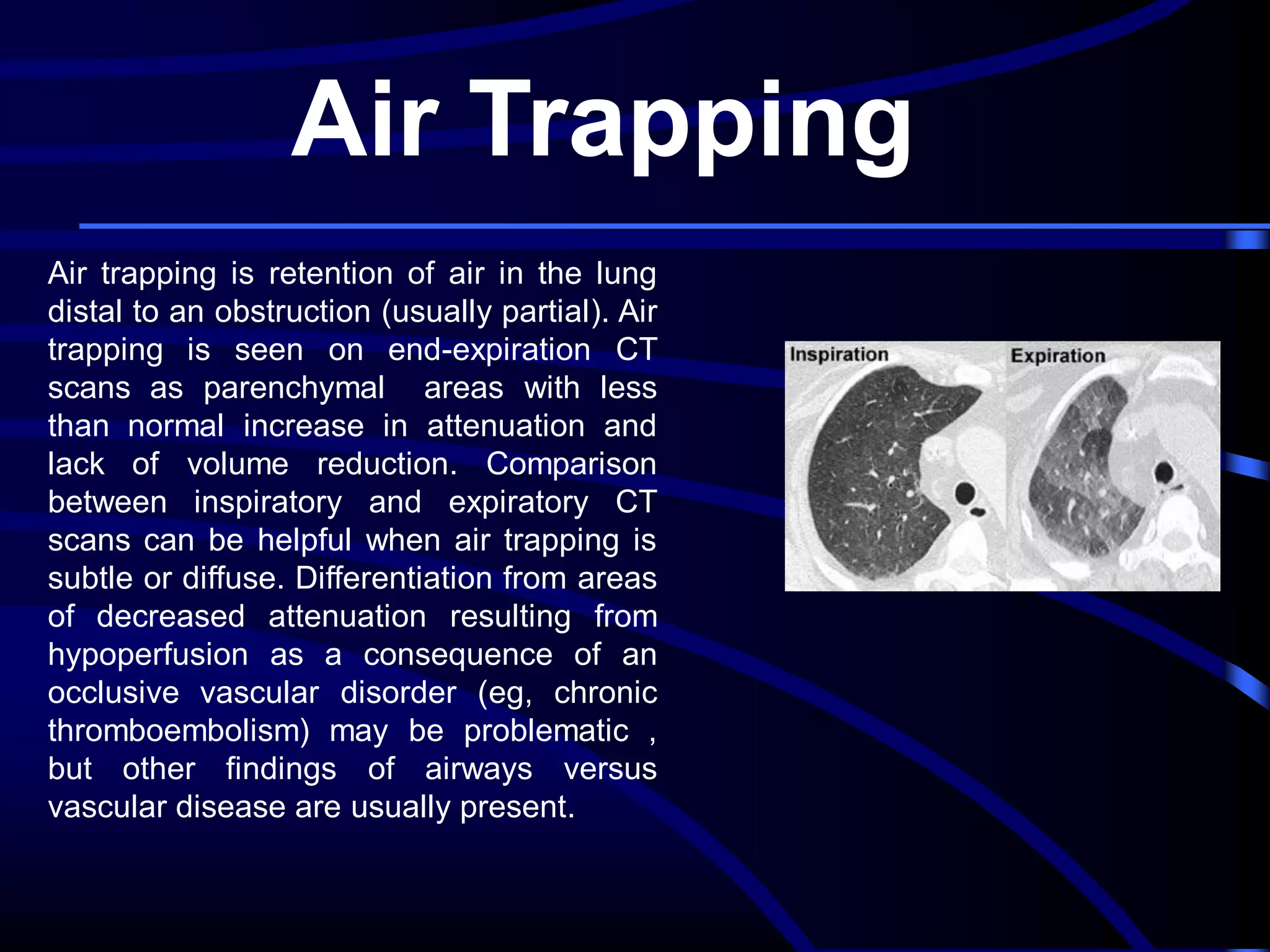
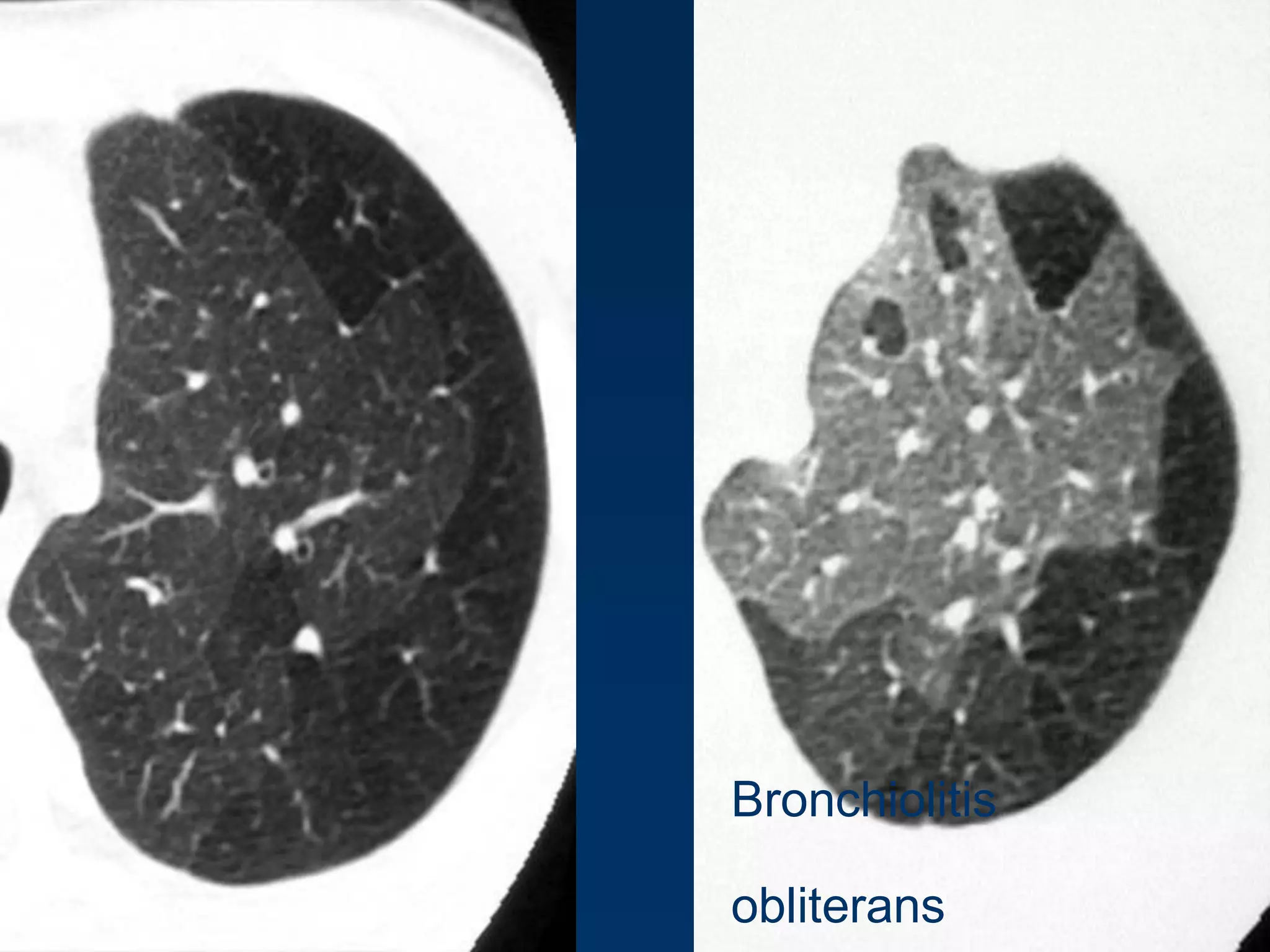
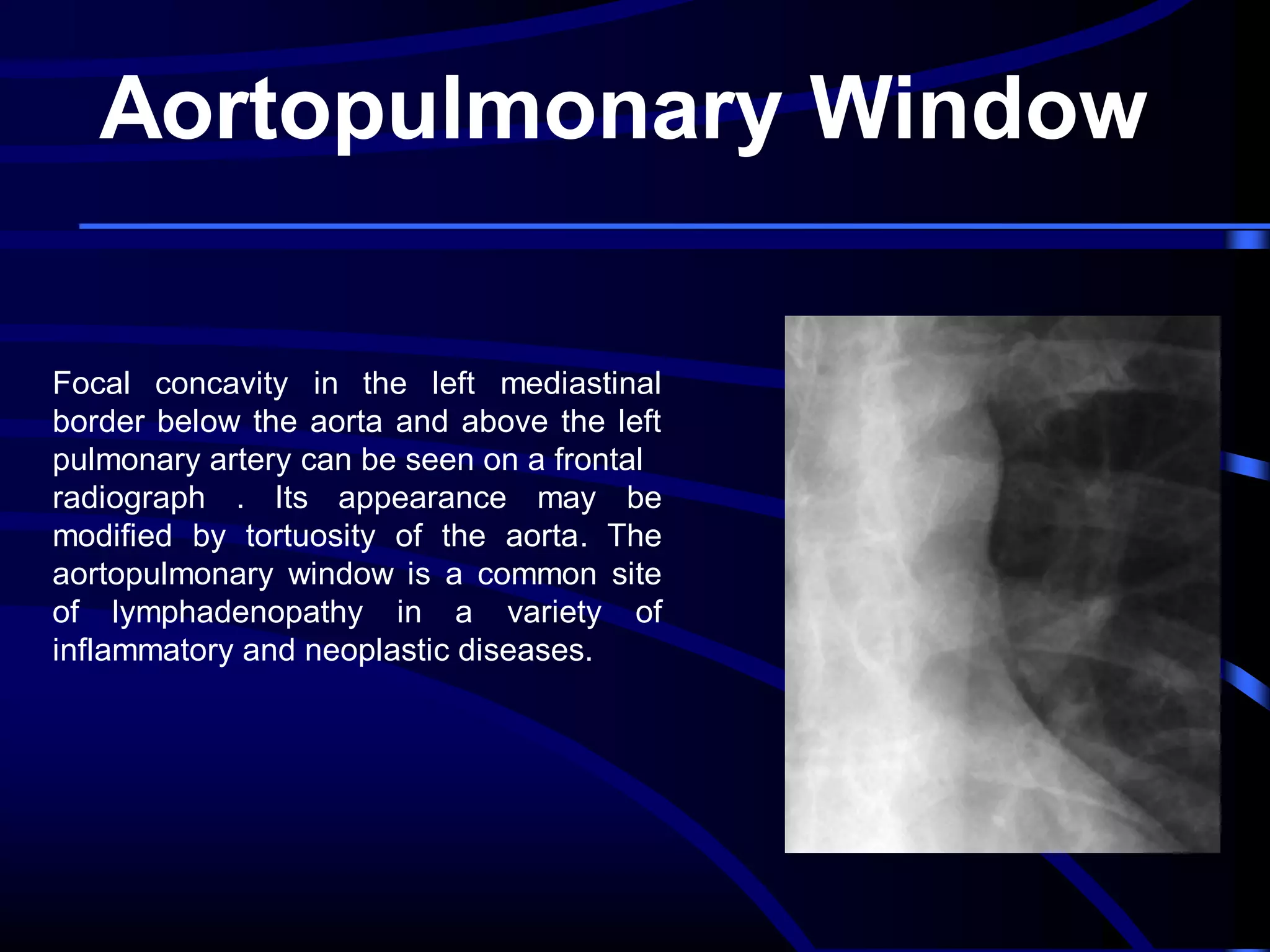

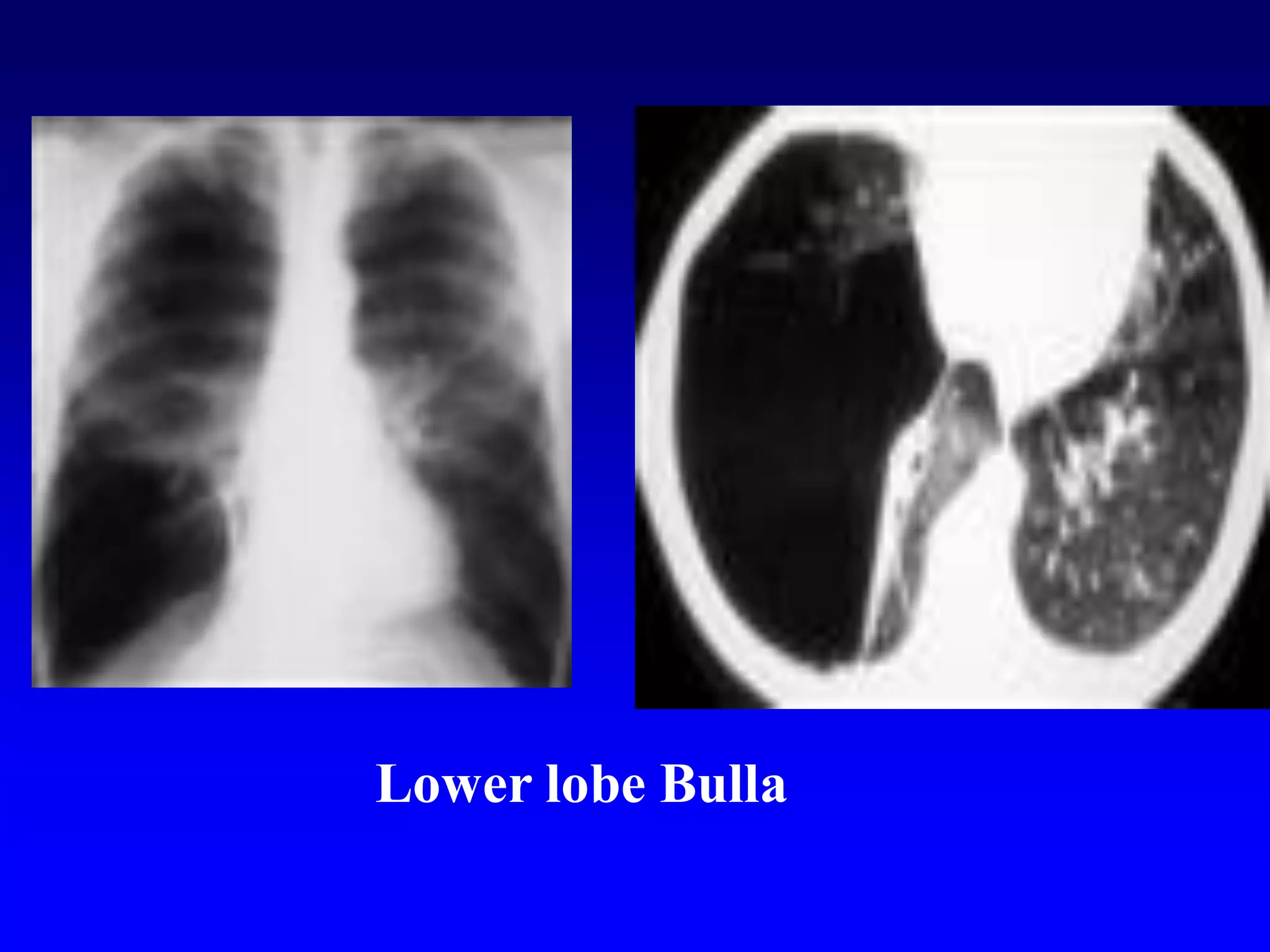
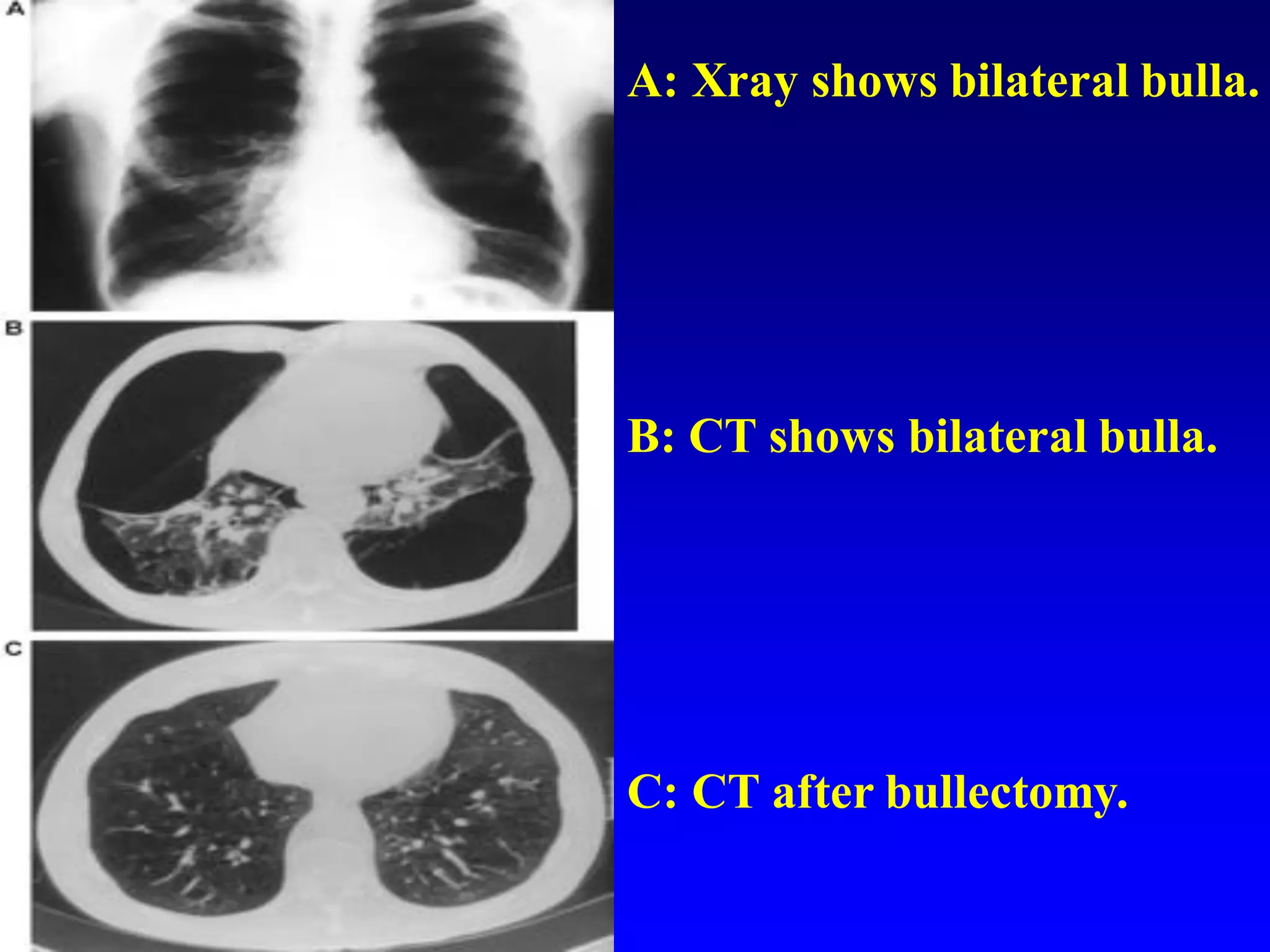
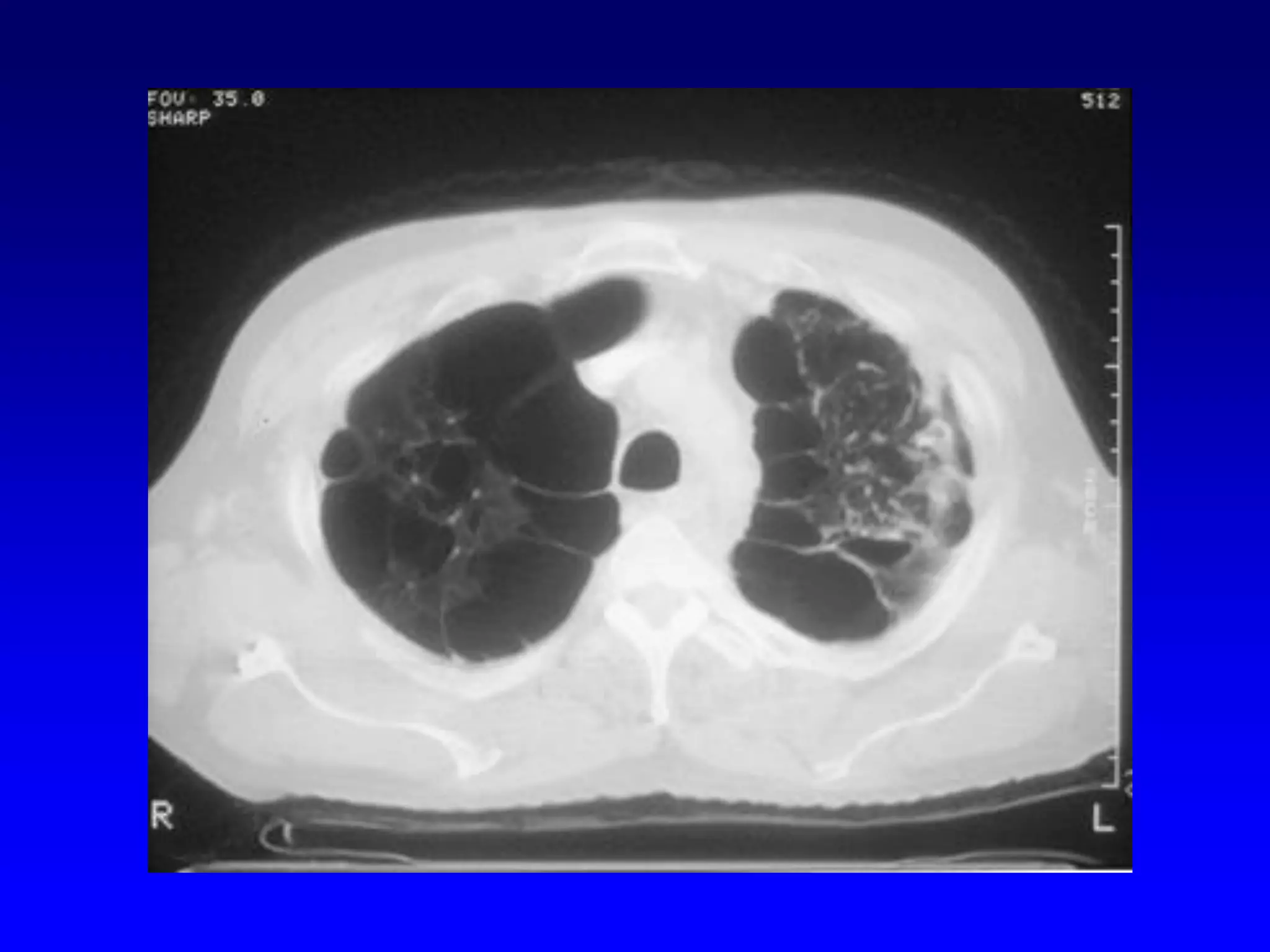

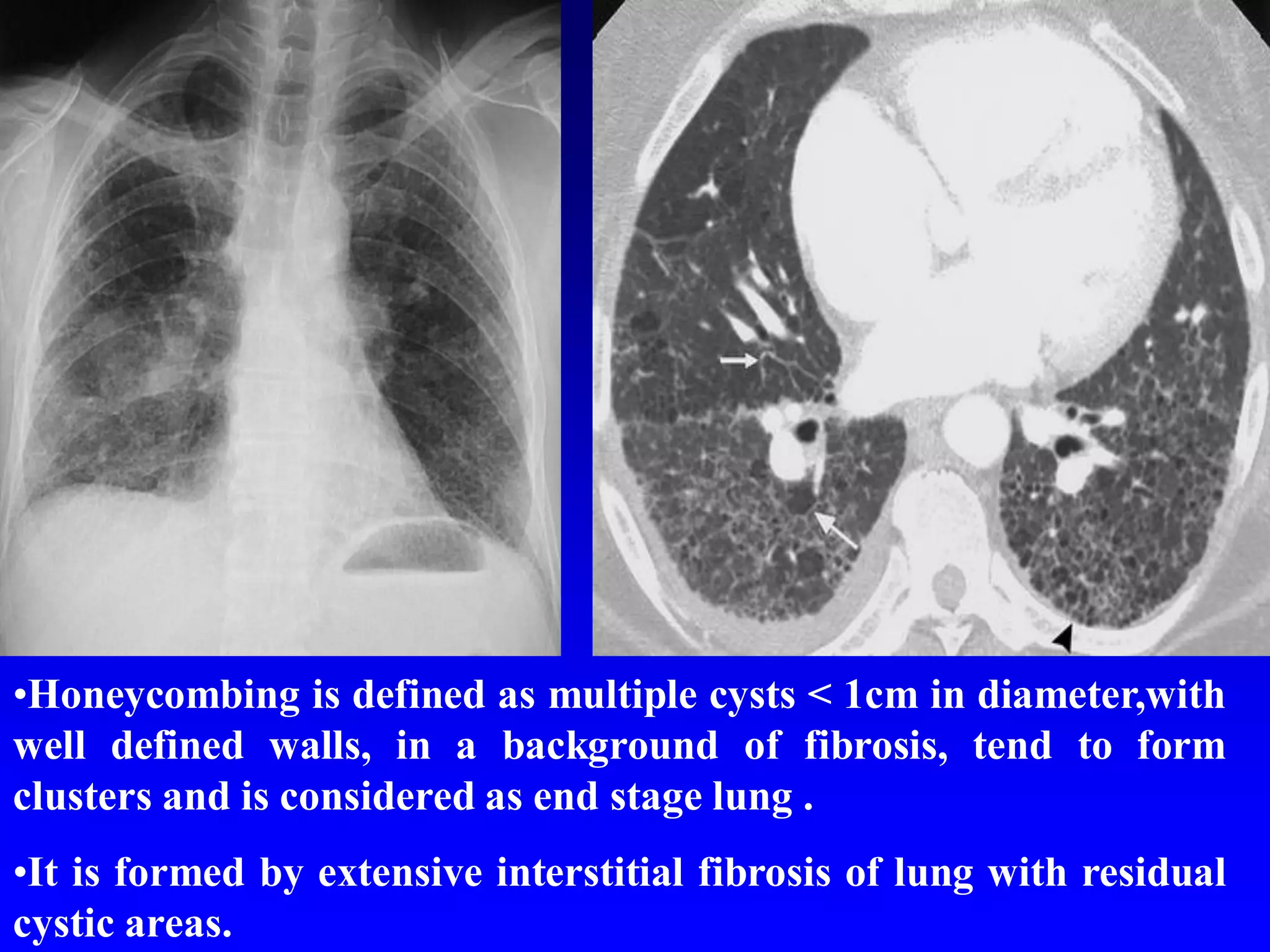


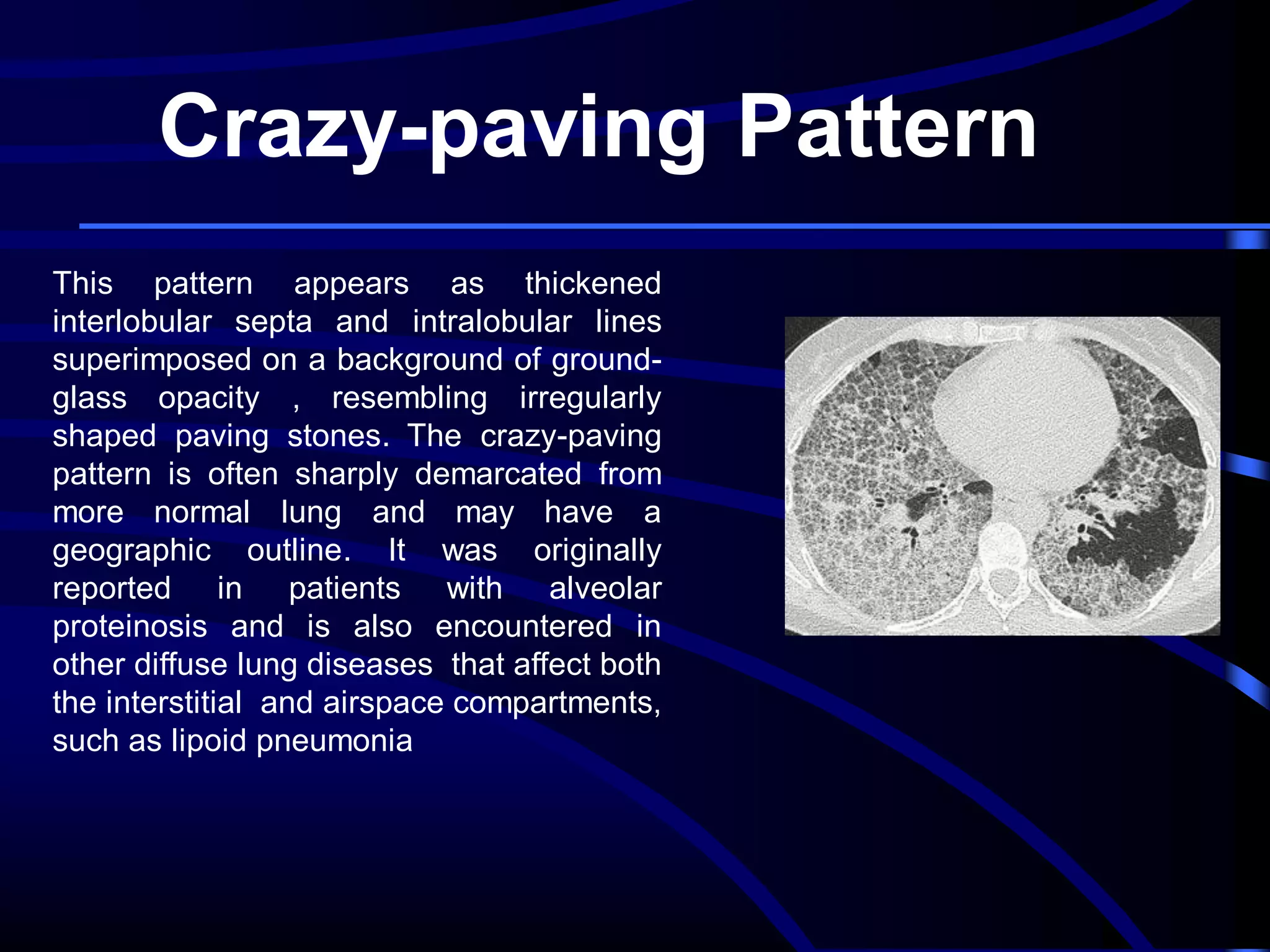
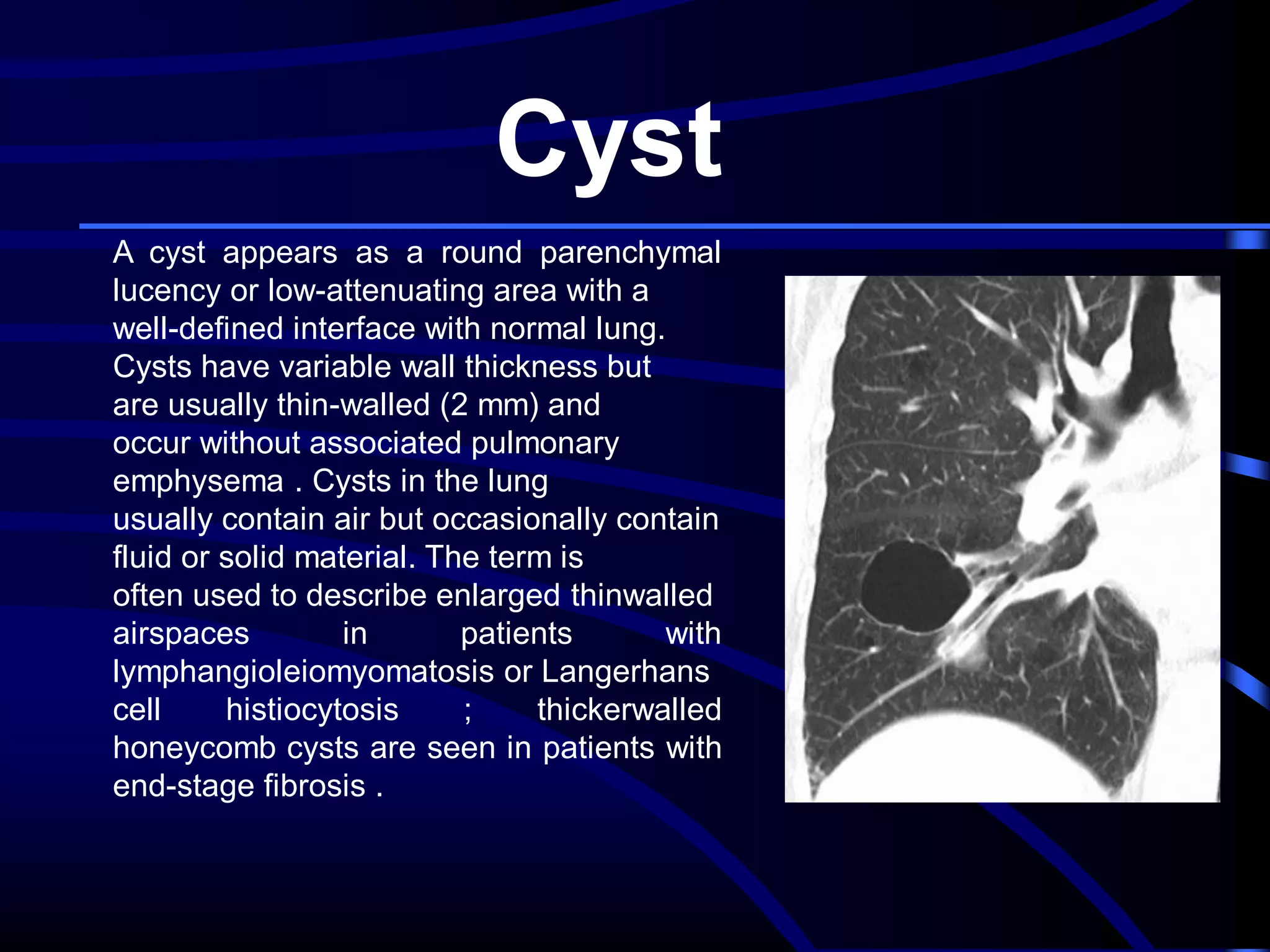
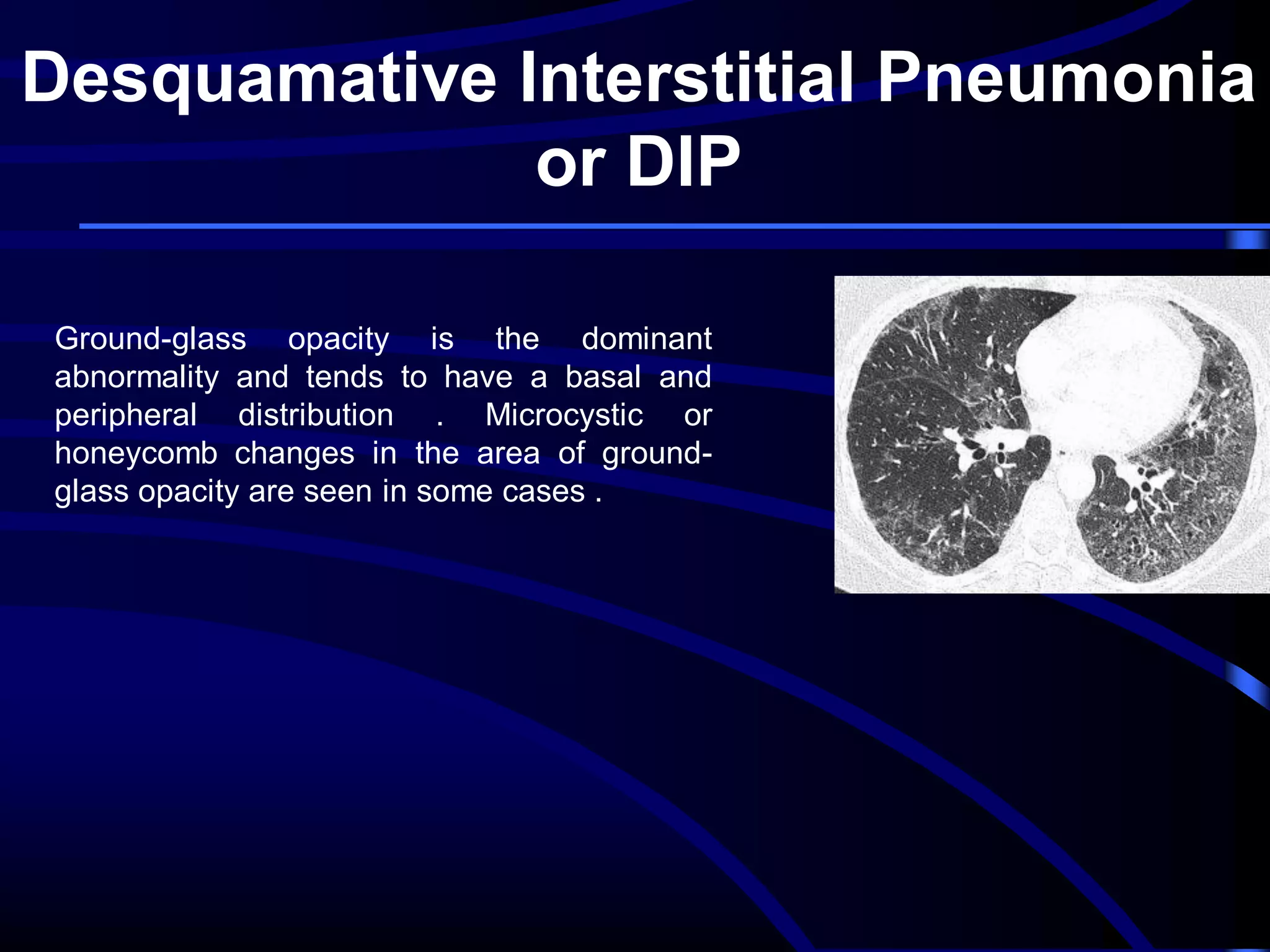
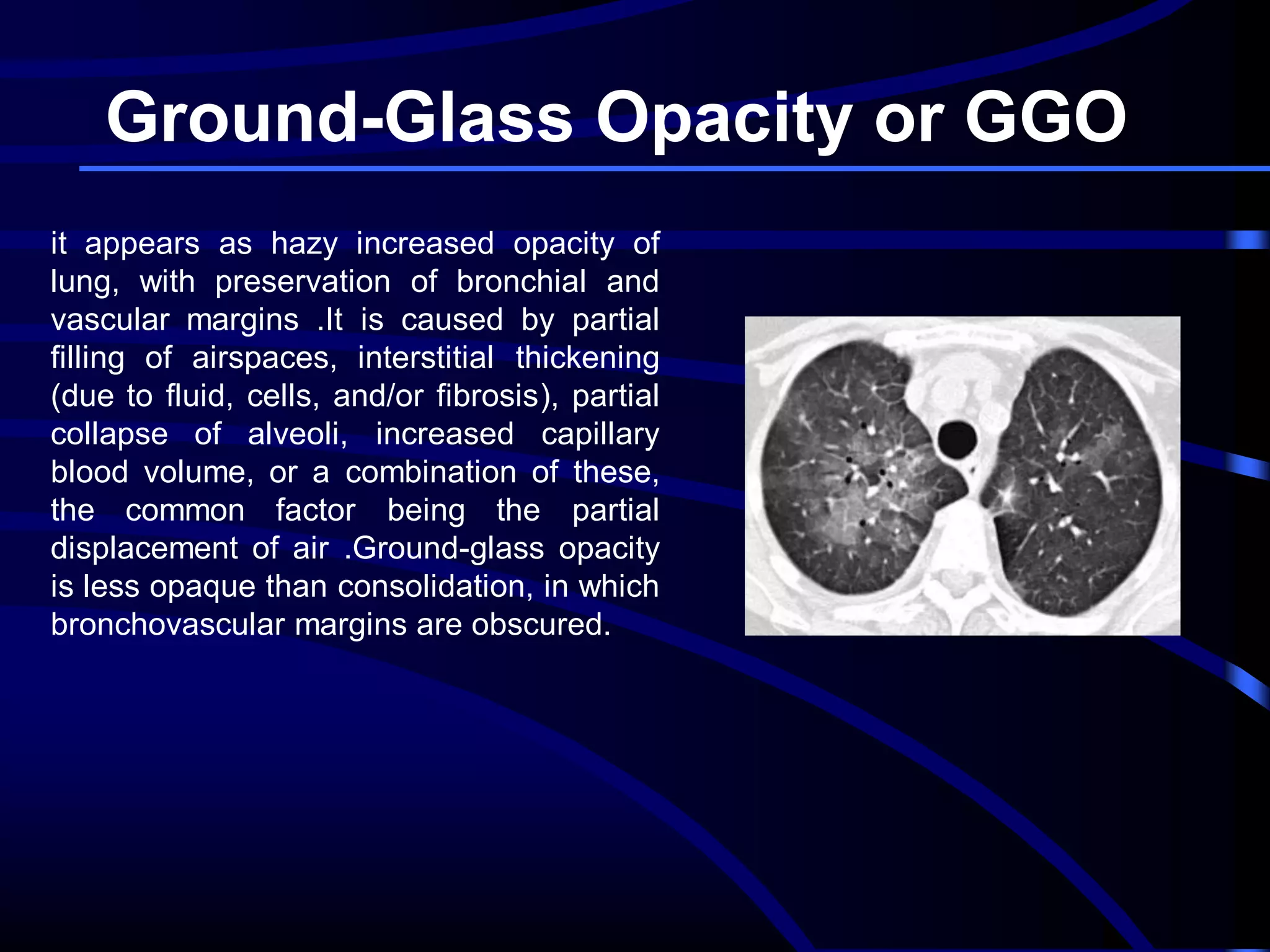




This document defines and describes various thoracic imaging terms related to the lungs. It discusses air bronchograms, air crescents, air trapping, and other terms. For each term, it provides a definition and brief explanation of what the term refers to in radiographic images of the lungs. The document is intended as a reference for radiologists and others to understand common findings seen in chest x-rays and CT scans related to lung pathology.











































































































