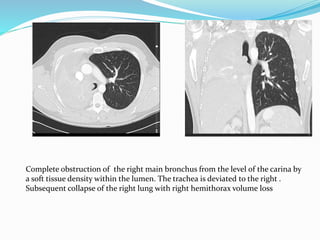
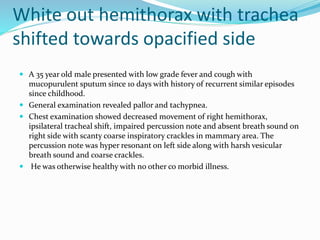
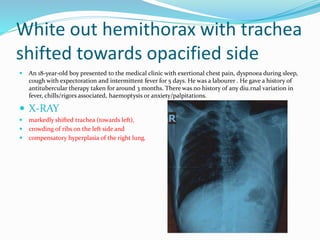
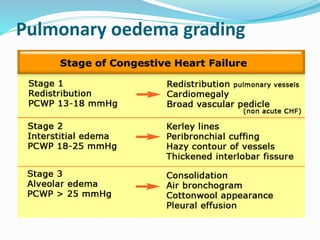
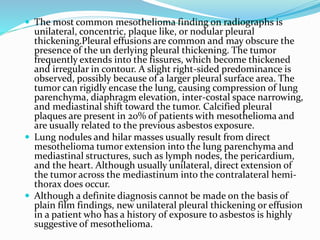
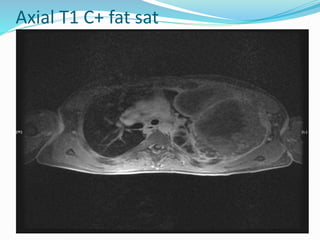
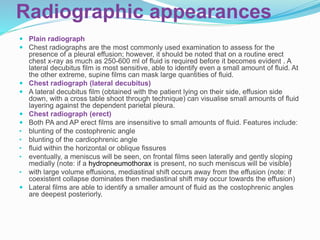
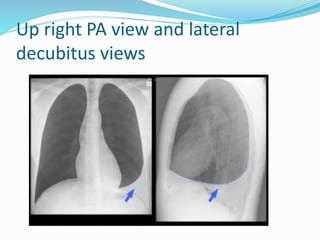
This document discusses the radiographic findings of complete opacification of one hemithorax seen on a chest x-ray. It notes that the position of the mediastinum and trachea can help narrow the differential diagnosis. Specifically:
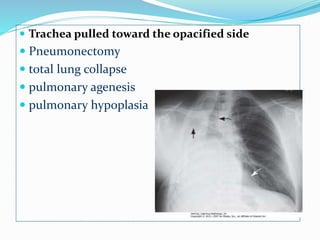
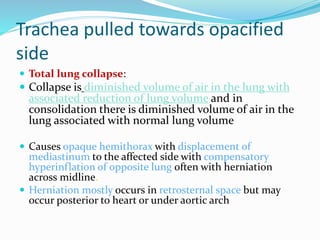
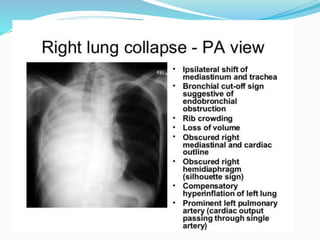
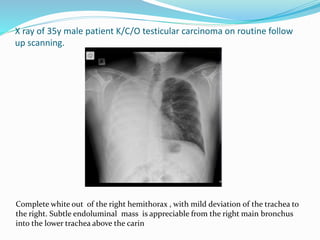
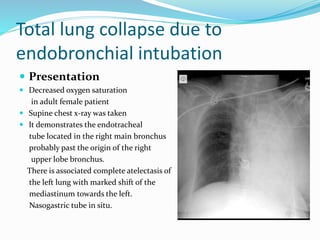
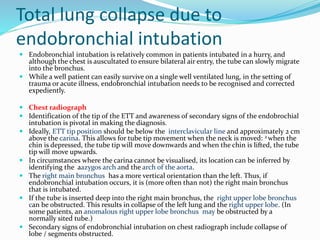
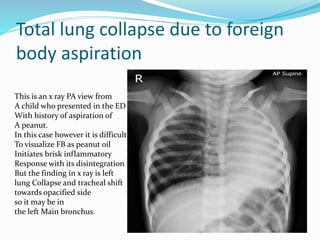
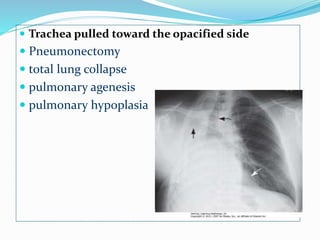
- If the trachea is pulled towards the opacified side, possibilities include pneumonectomy, total lung collapse, pulmonary agenesis, or pulmonary hypoplasia.
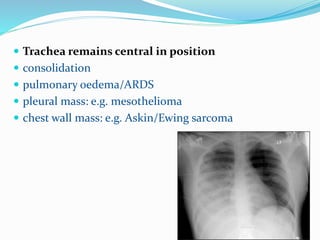
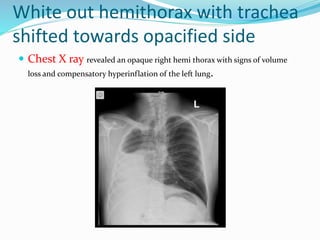
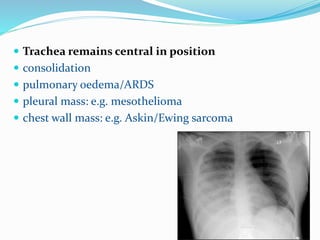
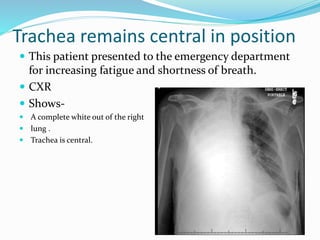
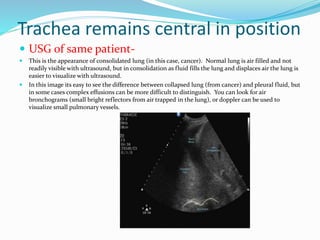
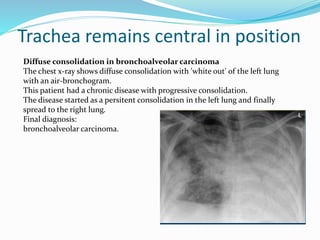
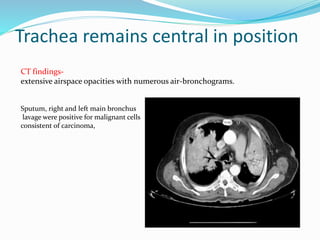
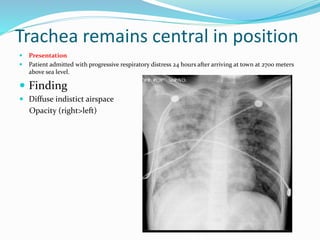
- If the trachea remains central, consolidation, pulmonary edema/ARDS, a pleural mass, or chest wall mass should be considered.
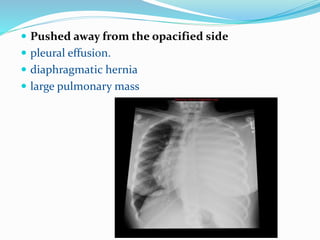
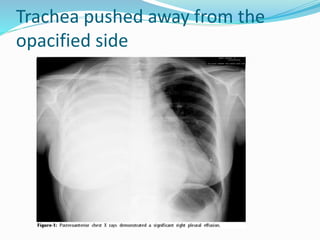
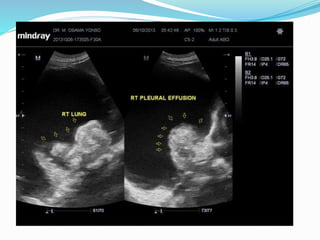
- If the trachea is pushed away from the opacified side, a pleural effusion, diaphragmatic hernia,







![Imaging in opaqe hemithorax [autosaved]](https://image.slidesharecdn.com/imaginginopaqehemithoraxautosaved-161030071708/85/Imaging-in-opaqe-hemithorax-autosaved-69-320.jpg)
![Imaging in opaqe hemithorax [autosaved]](https://image.slidesharecdn.com/imaginginopaqehemithoraxautosaved-161030071708/85/Imaging-in-opaqe-hemithorax-autosaved-70-320.jpg)








































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









