Download as PDF, PPTX


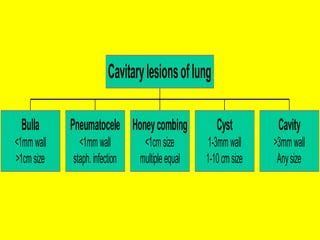
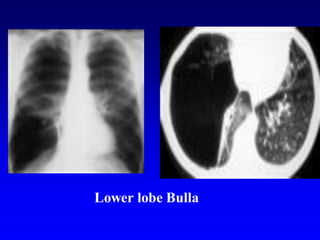
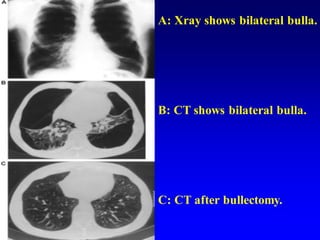
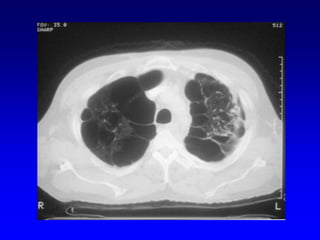
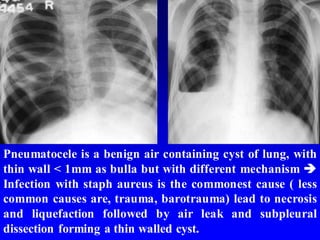
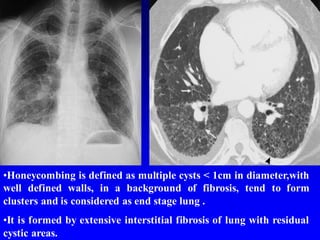
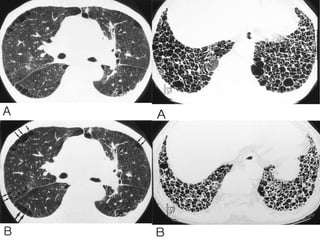








































Gamal Rabie Agmy, MD provides definitions and descriptions of various cavitary lung lesions and cystic mediastinal structures in 3 sentences or less: Bullae are thin-walled air spaces greater than 1 cm in size that result from destruction and dilatation of distal airspaces. Pneumatoceles are thin-walled lung cysts less than 1 mm thick resulting from staph infection and necrosis. Honeycombing describes multiple cysts less than 1 cm in diameter in a background of fibrosis, representing end-stage lung disease.











































































































