Downloaded 116 times





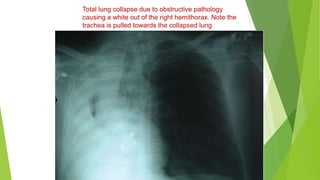
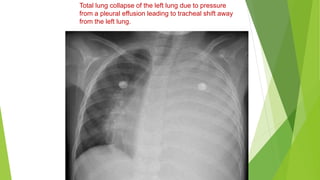




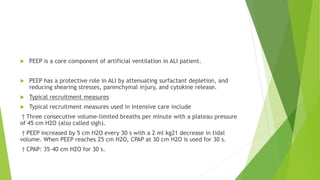
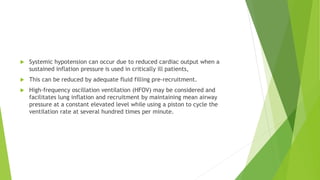
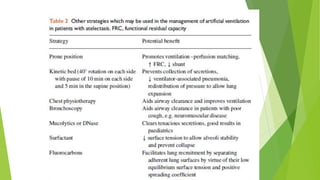

This document discusses pulmonary atelectasis, which is the collapse of lung tissue. It can occur during general anesthesia and in critically ill patients. During anesthesia, atelectasis is commonly caused by compression of the lungs or absorption of oxygen, while in critically ill patients it may be due to acute lung injury or surfactant depletion. The effects of atelectasis include decreased lung compliance and impaired oxygenation. Prevention techniques include positive pressure ventilation with PEEP and recruitment maneuvers. Treatment involves techniques to reopen collapsed lung regions.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






