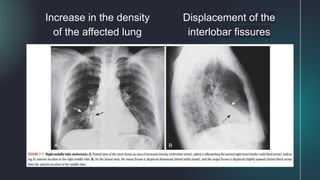
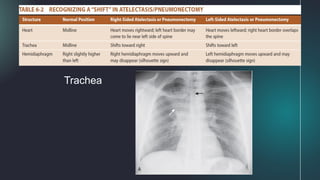
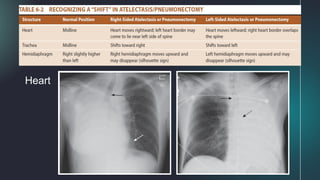
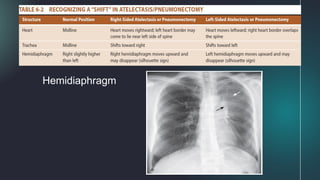
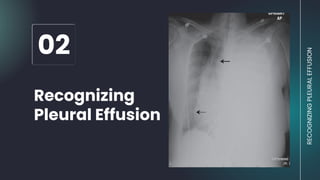
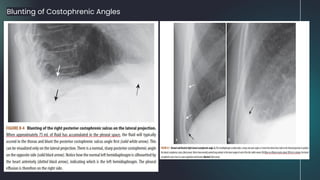
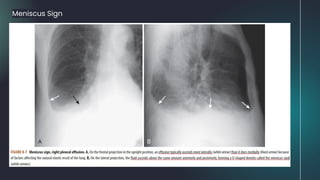
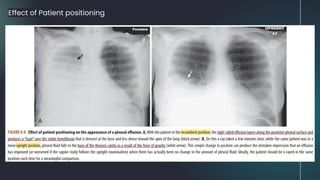
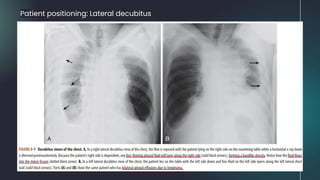
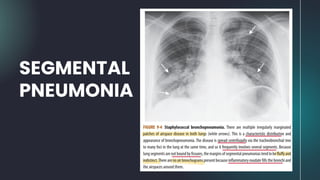
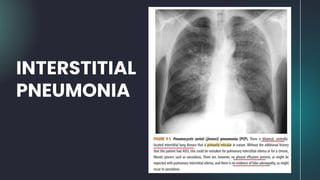
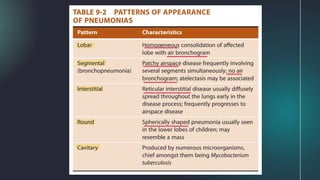
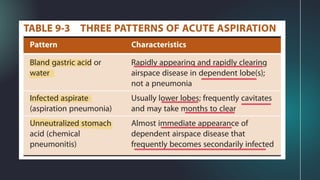
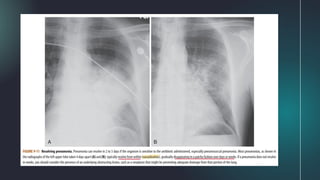
This document provides information on recognizing three common lung conditions: atelectasis, pleural effusion, and pneumonia. It describes the signs and patterns of each condition, including how they appear on chest x-rays. For atelectasis, it outlines different types like subsegmental and compressive atelectasis. For pleural effusion, it discusses characteristics like transudate vs. exudate effusions and how they can be positioned in the lungs. Pneumonia types covered include lobar, segmental, interstitial, round, and cavitary patterns. Localization clues and resolution of these conditions is also addressed.