Downloaded 50 times



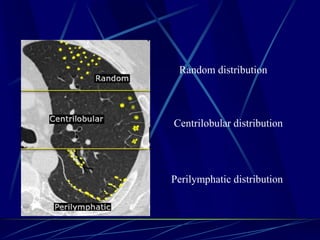
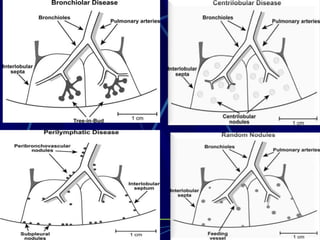
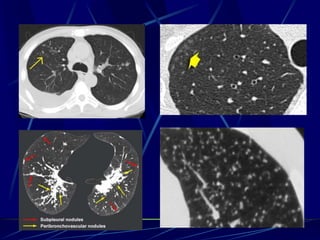
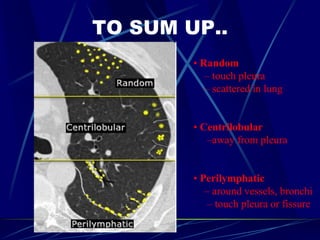
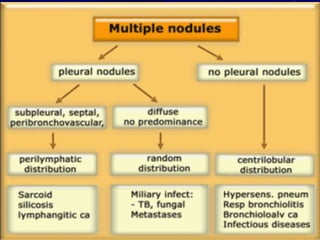
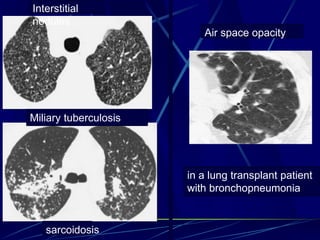
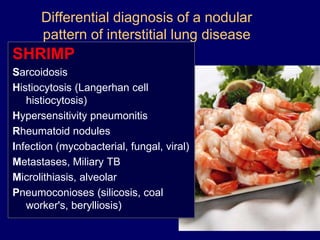
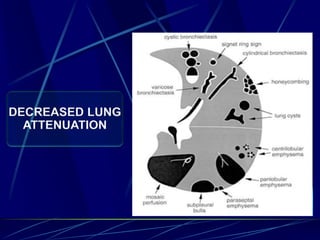
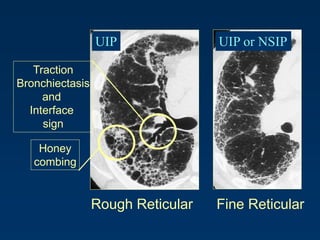
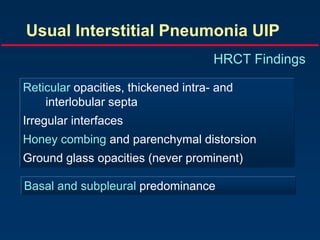
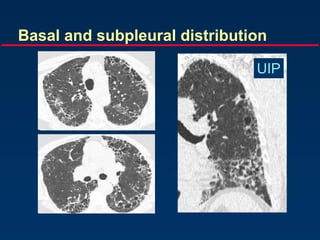
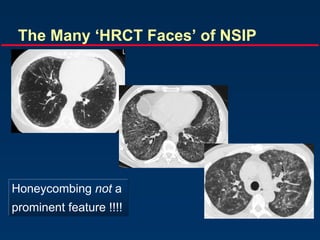
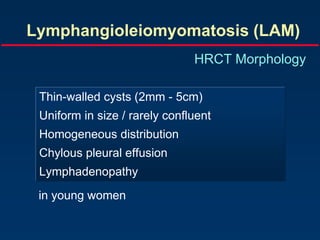
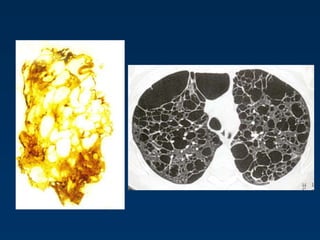
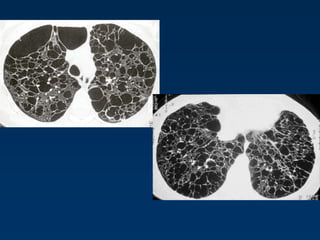
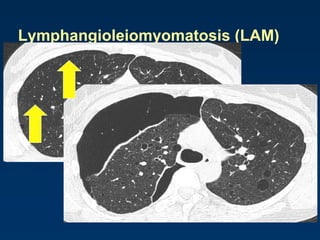
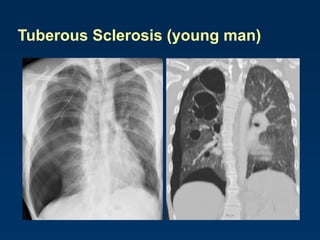
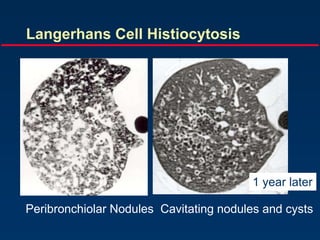
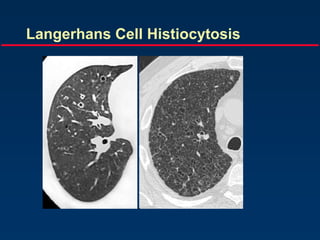
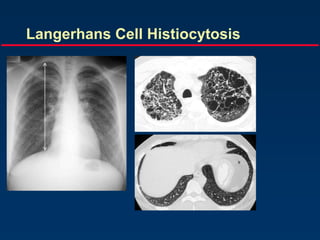
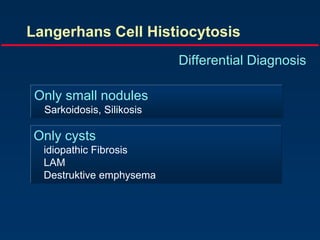
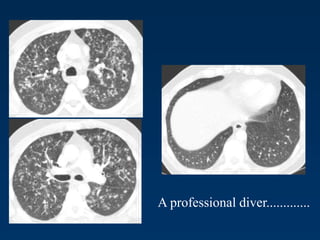
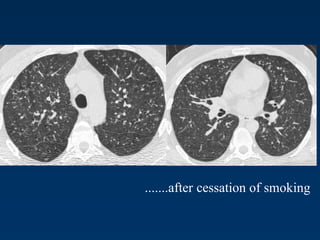

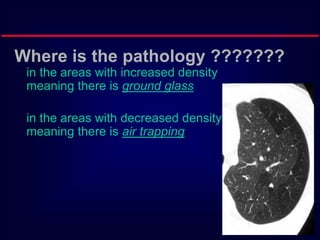
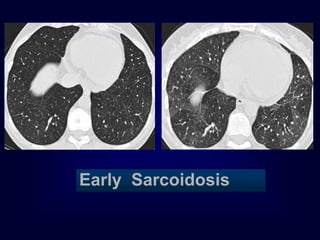
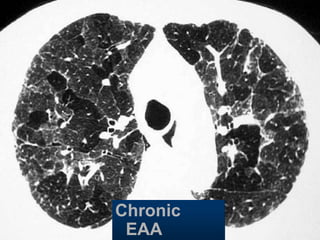
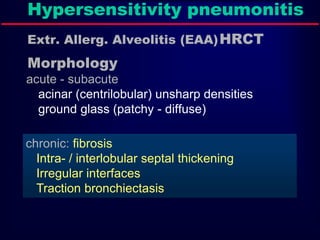
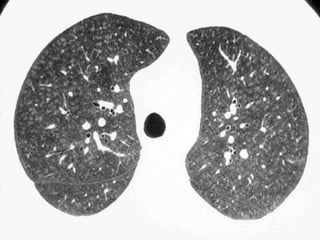
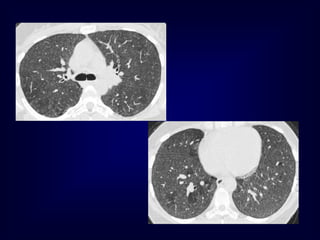
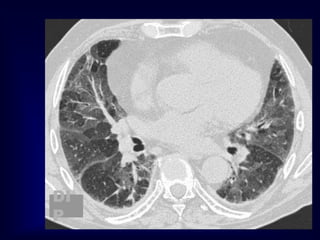
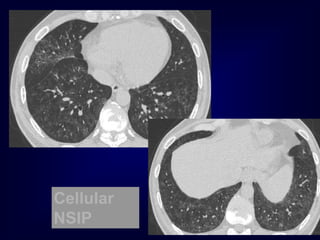


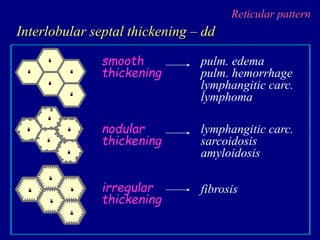
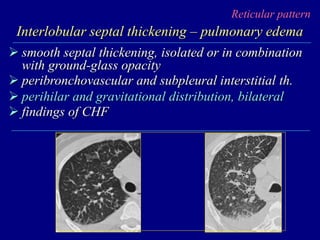
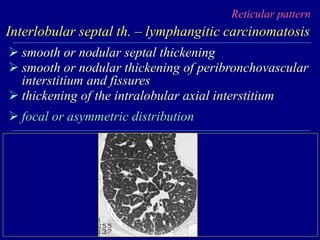
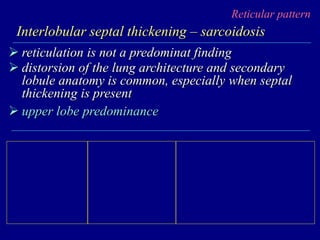
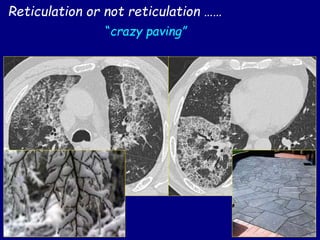
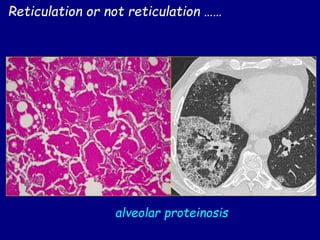
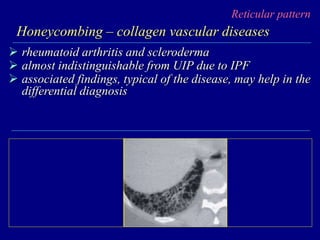
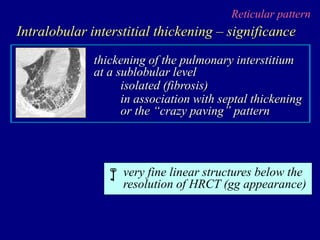
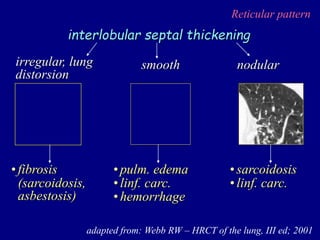
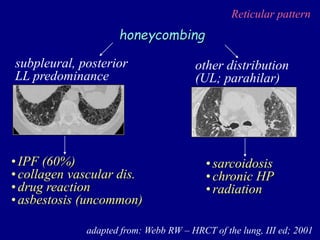
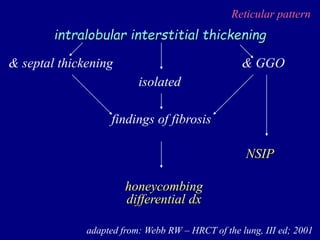
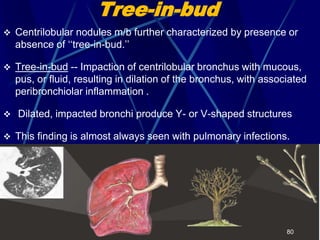
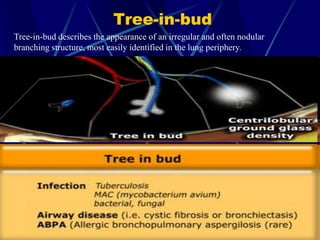
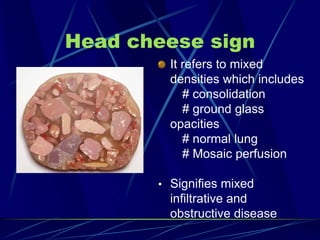


- The document discusses various patterns seen on HRCT scans of interstitial lung diseases including nodular, reticulation, cystic and tree-in-bud patterns. - It describes the significance of different patterns and features such as distribution of nodules, characteristics of interlobular septal thickening, honeycombing and intralobular interstitial thickening. - Differential diagnoses are discussed for each pattern to determine likely disease processes such as pulmonary fibrosis, infections, lymphangitic spread of cancer or sarcoidosis.



































































