1) Radial nerve palsy can be classified as high or low lesions, with high lesions demonstrating total loss of wrist extension in addition to finger and thumb losses.
2) Tendon transfers are commonly used to restore wrist, finger, and thumb extension when radial nerve function cannot be recovered. Jones pioneered many tendon transfer techniques still used today.
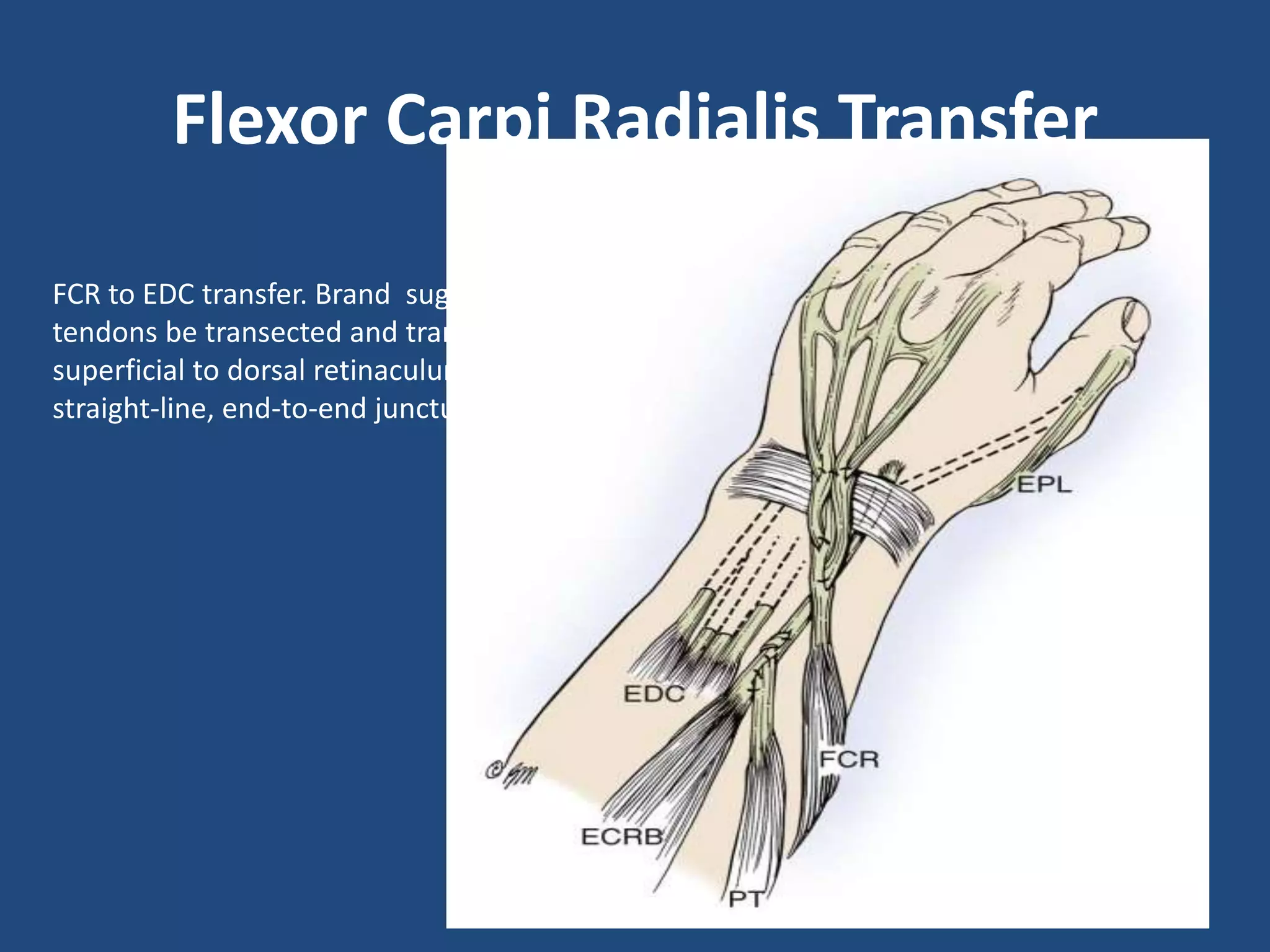
3) Common tendon transfers include the palmaris longus to the extensor pollicis longus to provide thumb extension and abduction, the flexor carpi ulnaris to the extensors digitorum communis to provide finger extension, and the pronator teres to the extensor carpi radialis brevis to provide wrist




![Requirements in a Patient with Radial
Nerve Palsy
• A patient with irreparable radial nerve palsy
needs to be provided with
(1) wrist extension.
(2) finger (metacarpophalangeal [MP] joint)
extension.
(3) a combination of thumb extension and
abduction.](https://image.slidesharecdn.com/tendontransferforradialnervepalsy-151117024050-lva1-app6892/75/Tendon-transfer-for-radial-nerve-palsy-6-2048.jpg)