Dr. Gavinash Rao presented on the history and techniques of tendon reconstruction. The history of tendon repair before 1960 primarily involved single-stage free tendon grafting. In the 1960s, two-stage reconstruction using silicone implants was developed. Currently, the Hunter technique uses a silicone rod implant in the first stage followed by tendon grafting in the second stage. Primary tendon repair is preferred if possible, while reconstruction uses tendon grafts from the palmaris longus, plantaris, or toe extensors. Complications can include adhesions, implant failure, and joint contractures.
Hand rehabilitation following flexor tendon injuriesAbey P Rajan
hand rehabilitation following flexor tendon injuries include introduction, clinical anatomy, tendon nutrition, tendon healing, post op. management, special cases, summary
Hoffa's Fracture: Diagnosis, management & New Classification System by BAGARI...Vaibhav Bagaria
Hoffa's Fracture - coronal split fracture of distal femur, its diagnosis, management strategy, a new classification and tips and tricks of management. First described Hoffa, a new classification system by Bagaria et al helps plan the surgery for these tricky fracture. The most crucial step is not to miss these fractures in ER.
Hand rehabilitation following flexor tendon injuriesAbey P Rajan
hand rehabilitation following flexor tendon injuries include introduction, clinical anatomy, tendon nutrition, tendon healing, post op. management, special cases, summary
Hoffa's Fracture: Diagnosis, management & New Classification System by BAGARI...Vaibhav Bagaria
Hoffa's Fracture - coronal split fracture of distal femur, its diagnosis, management strategy, a new classification and tips and tricks of management. First described Hoffa, a new classification system by Bagaria et al helps plan the surgery for these tricky fracture. The most crucial step is not to miss these fractures in ER.
Fractures and fracture dislocations of the tarsometatarsal jointMurugesh M Kurani
Here I have discussed an article from Journal of Bone and Joint Surgery. The presentation includes classification, treatment, results and complications. Lets share and learn.
Treatment of displaced midshaft clavicle fracture with locking compression plate provides better biomechanical stability, good fracture union rates, high post-operative constant score, early pain resolution, early return to activity, high patient satisfaction rates and excellent functional outcome. These benefits of plating overweigh complications when used in specific indications like displaced with or without comminuted middle third clavicle fracture (Robinson Type 2B1, 2B2).
A prospective observational study on comparing the outcome of patellar resurf...Dr.Avinash Rao Gundavarapu
Introduction: Total Knee Arthroplasty (TKA) has been a very successful surgery in relieving pain and restoring function in osteoarthritis. Conflicting evidence in literature exists regarding the merits of patellar resurfacing during TKA over non-resurfacing. Our aim is to evaluate and compare the difference between patellar resurfaced group and non-resurfaced group in primary TKA.
Materials and Methods: This prospective obsevational study was initiated in May 2016 conducted till April 2008 (2 years) in Yashoda Superspeciality Hospital, Hyderabad. At least 14 mm of patella was ensured to be retained after patellar cut. A total of 40 patients were allocated to receive (n=20) or not to receive patellar resurfacing (n=20) during primary TKA. The data was analyzed statistically using the Student t test. Overall patient satisfaction was recorded using the SF-36 score.
Results: Of the 40 patients, 67.5% females and 32.5 % males underwent TKA. Among those who underwent resurfacement, 40% were males. 75% among the non-resurfaced group were females. Right knee was operated on 37.5% of cases. Mean operative time being 103.9 and 122.5 minutes in nonresurfaced and resurfaced cases respectively. Mean patellar thickness was 22.1mm in nonresurfaced and 23.6mm in resurfaced group. The difference in VAS score, modified HSS score, KSS scores between the two groups were statistically insignificant with p-values of 0.230, 0.0214, 0.2513 respectively at the end of two year,
but there was significant reduction of anterior knee pain in the resurfaced with p-value < 0> Conclusion: The functional outcome was not affected by whether the patella was resurfaced or nonresurfaced. There was no significant difference between the two groups with respect to the prevalence of knee-related readmission, or of subsequent patella-related surgery or patients overall satisfaction. We recommend selective patellar resurfacing at the time of primary total knee replacement.
Keywords: TKA, Patellar resurfacement, Non-resurfacement, HSS score, KSS score.
Background
Traditionally, metallic interference screws were considered to have increased resistance to load than bio absorbable screws in anterior cruciate ligament (ACL) reconstruction. We did a comparative evaluation of biodegradable and metallic interference screws for tibial sided ACL reconstruction and also analysed complications, compared clinical outcome, did imaging study of ACL single bundle reconstruction by using titanium & newer poly–L-lactic acid (PLLA) bio absorbable screws to determine as to whether bio absorbable screw which costs double the metallic screw, is functionally better than standard metallic screws.
Methods
This is a prospective comparative study conducted among 50 patients aged between 15 and 55 years with clinical and MRI confirmation of complete ACL tear, treated arthroscopically with ACL reconstruction with either bio absorbable (group 1) or metallic (group 2) interference screw and both the groups were compared on follow up for an average duration of 12 months. Lysholm and Gillquist Knee Scoring Scale were used and outcome scores were divided into excellent, good, fair and poor.
Results
In our study 41 patients were males and 9 were females. Bio screw was used in 24 males and 6 female patients. Metallic screw was used in 17 males and 3 females. Outcome score was excellent in 26 (52 %) cases, good in 18 (36 %) cases, fair in 4 (8 %) cases, poor in 2 (4 %) cases. The mean Lysholm score in bio absorbable group was 93.13 and in metallic group was 89.70. Knee effusion was higher in bio screw group and infection rate was higher in metallic group.
Conclusions
In our study, the difference between bio absorbable screw group and metallic screw group was insignificant with regard to final patient outcome. Final osseointegration was better with bio absorbable screw, but increased cost of implant and almost same results compared to metallic screw does not make the bio absorbable screw superior to its counterpart.
Background: Distal femur fractures make up 6 to 7% of all femur fractures. Various plating options for distal femur fracture are conventional buttress plates, fixed-angle devices, and locking plates. This study was planned to evaluate and explore locking compression plate fixation in distal end femur fractures which is expected to provide a stable fixation with minimum exposure, early mobilization, less complications and a better quality of life.
Methods: The study was conducted as prospective clinical study in 20 skeletally mature patients with x-ray evidence of distal femur fracture fulfilling inclusion and exclusion criteria, operated with distal femur LCP plating. Patients were assessed radiologically and classified according to distal femur fracture classification and outcome graded as excellent, good, fair and poor based on Lysholm Knee Score.
Results: Out of 15 excellent outcome cases, 3 cases were type A1 fracture, 1 case had type A3, 2 cases had type B1 and B2 each, 5 cases had type C2 and 2 cases had type C3 fracture. 1 case with good outcome was type C3. 1 case with fair outcome was type B2. While 3 cases with poor outcome were type A1, A2 and C3.
Conclusions: The DF-LCP is an ideal implant to use for fractures of the distal femur. However, accurate positioning and fixation are required to produce satisfactory results. We recommend use of this implant in Type A and C, osteoporotic and periprosthetic fractures.
Keywords: Distal femur, DF-LCP, Lysholm score, Periprosthetic fracture
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
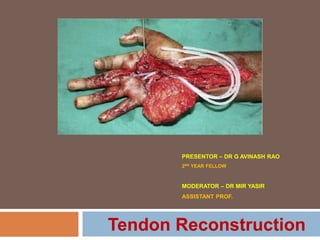
1. PRESENTOR – DR G AVINASH RAO
2ND YEAR FELLOW
MODERATOR – DR MIR YASIR
ASSISTANT PROF.
Tendon Reconstruction
2. HISTORY – Before 1960’s
In the tenth century, Avicenna, an Arabian surgeon, was credited with
performing the first tendon repair surgery.
In Europe, Galen teachings resulted in infrequent tendon repair. Galen did
not differentiate between nerves and tendons.
Historically, one of the first experiments on flexor tendon reconstruction -
described in 1910 by Lange - strengthened the transplanted tendon with
strands of silk impregnated with paraffin - did not have favourable results-
post-operative adhesions.
3. In 1936, Carl Henze and Leo Mayer - a novel technique for the restoration of the
digital sheath using celloidin tubes -mto provide a gliding.
Until the 1960s, tendon lacerations in zone 2, or “no man’s land,” - treated with
removal of the tendon with grafting of new tendons.(Sterling Bunnell teachings)
4. HISTORY – After 1960’s
Single-stage free tendon grafting - Pulvertaft, Graham, Littler, Boyes, and
Stark
In 1963, Bassett and Carroll first described - two-stage flexor tendon
reconstruction using a silicone implant.
In 1965, Hunter first published - tendon implants for tendon reconstruction.
He further refined his work in 1970s using Hunter silicone rod - staged
tendon reconstruction technique - currently used.
5. Paneva-Holevich in 1969, sutured the proximal cut end of the FDS to
the proximal cut end of the FDP in the palm.
At the second stage, the FDS tendon was severed proximal and this
end was brought out to be inserted at the distal phalanx as a pedicle
graft.
In 1982, Paneva-Holevich - secondary repair of 324 flexor tendon
injuries using pedicle FDS tendon grafting.
15. Primary Tendon repair
Contraindications :-
1. Severe contamination with suspicion of wound infection,
2. Long defects of the tendons,
3. Extensive destruction of pulleys.
4. Serious crush injuries, extensive loss of soft tissues,
5. Fractures involving multiple bones, particularly at different levels.
6. Fractures which cannot be stabilized adequately by internal fixation,
7. Bony injuries involving joint components.
18. Primary tendon graft reconstruction (BUNNELL)
The outcomes are inferior to primary flexor tendon repair.
Prerequisites -
1. Well healed, stable, mobile soft tissue cover without extensive scarring.
2. With an adequate pulley system.
3. Passive movements are full, or nearly full.
4. At least one intact digital nerve
19. Indications
1. Injuries with segmental tendon loss.
2. Severe peritendinous tissue injuries at initial presentation.
3. Delay in repair > 3 to 6 weeks.
4. Suspicion of wound infection - percluding primary repair
5. Delayed presentation of closed FDP avulsion from the insertion with
significant retraction.
6. Closed rupture in zone 1 to zone 3, with retraction of the proximal
tendon that does not permit a direct end-to-end repair.
Primary tendon graft reconstruction (BUNNELL)
21. The best indication for single-stage free tendon graft for flexor tendon injury is
the grade 1 hand according to Boyes classification or according to Merle and
Dautel’s classification For grade 2 or 3 hands and above staged tendon
grafting is preferred.
22. Donor Tendons
Ipsilateral palmaris longus or plantaris tendons remain the most common
choices. (extrasynovial tendons)
Toe extensors from beneath the ankle retinaculum within the sheath and
Toe flexors are also intrasynovial; but their sheaths tend to be much
shorter than those of the fingers.
Vascularized tendon grafts have been described - rarely used and little is
written in literature.
23. Palmaris longus
Present in about 75-85% of population.
Lister said that it was absent unilaterally in 14% and bilaterally in
16% subjects.
PL agenesis differs according to race, sex, and to the right and left
side.
There is a wide variation in the incidence of PL ranging from 0% to
63% with an overall 16% unilateral and 9% bilateral absence
described in the literature.
29. Plantaris tendon
When multiple grafts / one long distal forearm-to-fingertip graft needed,
The presence cant predicted clinically, ultrasound or MRI can,
It is said to be absent in only 7% of cadavers,
Harvey and associates - tendon was present in only 80% of limbs.
Unusable sometimes because of variations in its girth / attachments to
the triceps surae, which make removal impossible.
30.
31. Long Toe Extensor Tendon
Presence is never in doubt, and diameter is adequate
Three long tendon grafts - second, third, and fourth toes
Individual tendons may fuse distal to the ankle.
Large longitudinal incision / Tendon stripper / multiple transverse incisions
Other options – EIP , FDL of foot can also be used
32.
33. Biology of Tendon graft
Incorporation
Intrasynovial donor tendons seem adapted to survive transplantation
to the digital sheath and can incorporate without the formation of
peritendinous adhesions - surface is designed to allow for synovial
fluid imbibition , promote nutrition and cellular survival.
Extrasynovial donor tendons undergo - peritendinous necrosis - with
the formation of dense peritendinous adhesions during tendon graft
incorporation - new vessels growing through adhesion formation and
the tendon junctures
40. In cases of disruption of both the FDP and FDS tendons, general
surgical principles for this procedure include:
1. Place only one graft in each finger.
2. Use a graft of a suitable caliber to fit into the finger.
3. Place the proximal junction outside the tendon sheath.
4. Avoid damage to the fingernail or fingertip, in making the distal
junction.
5. Ensure adequate graft tension.
Primary tendon graft reconstruction (BUNNELL)
41. In cases with an intact or functioning FDS tendon, the following
additional principles apply:
1. FDS-only fingers may have sufficient function without using free tendon
grafting to reconstruct the FDP tendon.
2. Never sacrifice an intact FDS or damage the surface of the FDS tendon
during surgery.
3. In young patients – Consider FDP grafting – After explaining risk of
worsening function.
4. Options – Tenodesis / Arthrodesis in Manual Labours & elderly.
5. Prefer in RF, LF @ Power Grip.
Primary tendon graft reconstruction (BUNNELL)
42. Post op Rehabilitation
Accelerated rehabilitation protocols.
Early active motion protocol is used for compliant patients.
Postoperative splint - static dorsal blocking splint, with the wrist in
neutral, the MP joints in 45 degrees of flexion, and the IP joints in
neutral worn for 6 weeks after surgery.
43. Two stage - Reconstruction
Indications - Considered in severe trauma
with extensive destruction of flexor pulleys,
with crushing injuries with extensive soft tissue damage and underlying
fractures,
with extensive scarring of the flexor tendon bed and Overlying skin.
Inadequate passive range of digital motion.
44. Hunter - is credited for his work with a goal of creating a new flexor
tendon bed allowing for gliding of the implanted tendon graft and
recreate a sufficient and functional pulley system.
Options exists for pulley reconstruction, include - Extensor retinaculum,
remnant of free tendon, FDS tendon, Volar plate or synthetic materials
like Dacron arterial graft, silicone rubber sheeting, xenograft materials,
polytetrafluoroethylene, woven nylon and fascia lata, and porcine
collagen and peritoneum.
45. The first stage includes reconstruction of the pulley and sheath system,
and the placement of the silicone rod as a temporary implant in the
tendon bed.
This is followed by a strict rehabilitation protocol to restore digital flexion
before secondary reconstruction 3–6 months afterwards.
The placement of the silicone rods (8, 10, 12,14 F – Corresponding to
diameter of FDS) leads to the development of a pseudosheath
(mesothelium) around the implant.
This allows for replacement of silicone implant with - tendon graft in a
functional bed - that prevents scar formation and soft tissue adhesions.
46. The pulleys should be carefully evaluated and prepared in order to
receive the graft.
When the pulleys are intact they can be dilated to allow tendon graft
gliding.
In cases with complete damage, the pulleys can be repaired,
reconstructed and tensioned.
The ideal tendon graft for the second stage reconstruction - should
have intrasynovial lining on the tendon gliding side.
47.
48.
49.
50. In the second stage the tendon graft is fixed to the distal end of the
previously implanted rod and pulled proximally through the
pseudosheath.
Then the implant is removed and discarded and the tendon graft is finally
sutured to the proximal intact flexor stump with correct tensioning.
51.
52. Complications of Tendon Reconstruction
Adhesion formation
Mechanical failure of implant
Graft rupture
Pulley Disruption
Quadrigia Syndrome
Lumbrical plus finger
Swan neck deformity
Infection
Synovitis
Late flexion deformity
53. Post operative
A short-arm posterior molded plaster splint from - fingertips to below the
elbow.
The wrist is maintained in neutral, the MP joints in 40 to 50 degrees of
flexion, and the IP joints in neutral.
Controlled active range of motion exercises under supervision of hand
therapist
54. Tendon Prosthesis - Hunter rod
Made of woven polyester core covered with barium impregnated silicone
elastomer.
This device is developed by Dr. James M. Hunter for the reconstruction
of flexor and extensor tendons.
Residual antecedent infection is a contraindication for the use of this
device.
Rod portion of the device is 4 mm wide and 2 mm thick and varies in
length, The cords extend 15 cm beyond the ends of the rod
55. Passive - distal end of the implant is fixed to bone or tendon & proximal
end glides freely in the proximal palm or forearm.
Active – Fixed both proximally and distally.
2 passive tendon implants available - differ only in their distal juncture.
One has a stainless steel distal metal end plate that is attached to the
distal phalanx by a screw.
Other has a screw-fixation terminal device is held in place with a 4-0
nonabsorbable suture to distal FDP stump.
57. Indications for an active tendon rather than a passive tendon:
(1) Patient with proper motivation & good compliance with rehabilitation
protocol,
(2) An extensor system that functions well enough to balance the
flexion,
58. Soft tissue and joint deficiencies
/scarring
Management - Individualized to each case.
Two staged procedure –
1. First stage – Soft tissue + joint deficiencies + pulley reconstruction + silicon
rod.placement.
2. Second Stage – Tendon grafting.
3. Might extend to third stage
Keep proximal stump away from the scarred / injured area. – Preffered at
Wrist Level.
59.
60.
61.
62. Modified Paneva - Holevich Technique
Prerequisite-
Injury to both FDP, FDS with serious scarring and a nonfunctional flexor
apparatus.
Indications
(1) Flexor tendon reconstruction in Boyes 2 to 5 injuries in zone 2 with
considerable scarring of the tendonbed;
(2) Finger replantation with damage to the fibroosseous canal;
(3) Failed previous flexor tendon reconstruction.
66. Advantages over Hunter
technique
(1) No need of identify motor during the first stage;
(2) The FDS-FDP loop - identified easily in palm - during the second
stage;
(3) There is no donor site morbidity (no free grafts)
(4) Performed easily in children;
(5) Pedicled tendon graft with a strong proximal junction - already healed
before second stage ;
(6) Uses FDS as graft that is consistent. (palmaris longus, plantaris,
which are reported to be absent in few)
67. (7) The FDS tendon graft is three times larger than conventional grafts
used in the Hunter technique – need thicker Silicone rod.
(8) FDS - intrasynovial graft – better graft incorporation than
extrasynovial grafts.
68. Disadvantages
The difficulty in tensioning the graft at the distal anchoring site of the
graft. The proximal tendon junction healed by this time.
The FDS of the little finger sometimes is thin in the wrist and cannot be
used.
This problem can be overcome by reinforcement of the tendon with a PL
graft or by using the FDS of an adjacent finger.
69. Complications
Flexion contracture of the DIP joint (most common) - treated with night
extension splints.
In First stage complications include (1) rod buckling, (2) necrosis of the
skin, (3) rod migration, (4) rupture of the distal end of silicone rod, (5)
synovitis, and (6) infection.
In second stage complications can be (1) bowstringing, (2) impingement
of the proximal suture in the fibro-osseous canal, (3) tendon grafts loose
or tight, (4) disruption at the distal or proximal junctions, (5) flexion
deformity of the proximal interphalangeal (PIP) and/or DIP joints, and (6)
infection.
70. Flexor tendon injuries in
children
In delayed cases - parents should be informed of the possibility for
grafting of the flexor tendon.
Immobilize with above elbow plaster cast for 1 month in <7 yrs
children – followed by active motion exercises
Defer Reconstruction (not repair) in < 7 years.
Bruners incision vs Midlateral incision (Absorbable sutures)
Bunnell pull out suture – avoid physeal damage.
Repair both FDP and FDS.
Avoid Plantaris as graft.
72. FPL reconstruction
Direct repair - possible - 3 to 4 weeks after injury but, there is sufficient
shortening of the muscle within a few days – Extended primary repair
with proximal tendon lengthening.
Delay of the repair beyond 3 to 4 weeks may cause myostatic shortening
of the muscle–tendon unit.
Primary repair in zone 3 is difficult – Matev (1983) – Tendon graft from
wrist – reconstruct FPL primarily in single stage.
Distal tendon dissection – Requires careful attention to digital NVB.
Zone 4 injury – immobilize wrist in neutral to slight extension – after
repairing sphagetti wrist and releasing Carpal tunnel. (Jin bo Tang).
73. FPL reconstruction
Indicated in failed repairs and Neglected injuries.
Prerequisite for grafting in stage 1 is adequate excursion on table
and intact Oblique pulley.
Incompetent pulley system and extensively scarrred bed with
adequate excursion – Two staged reconstruction.
No adequate excursion on table – Tendon transfer.
74.
75.
76. The distal vinculum brevis is present in 90% of thumbs and is strong.
If intact after injury at the level of the IP joint, it will retain the FPL within
the thumb.
Pulvertaft thought that local adhesions played a part in maintaining the
tendon in the thumb.
The FPL has a functional amplitude of excursion of 5.5 to 6 cm:
If the amplitude of excursion of the cut end of the proximal tendon is far
short - using it as a motor for reconstruction will not achieve IP joint
flexion.
77. Matev - Rule of thumb : FPL Reconstruction.
If the passive stretch of the muscle fibers, measured at the wrist, is 3 to
4 cm, full restoration of function may be expected.
Even with 1.0 to 1.5 cm of passive stretch, the result is likely to be
adequate. If less than this, he advised using another motor.
78. Tendon grafting in FPL
Reconstruction
Bridge grafts from Wrist to distal phalynx planned / Thenar tunneling /
Distal attachment / proximal attachment
Tension adjustment – Schneider (1999) detailed a more precise setting
of the wrist at 0°, the thumb abducted in front of IF metacarpal, and IP
joint of thumb in 30° of flexion.
Matev suggested the IP joint be set at 20° to 30°.
Tendon Transfer – FDS of RF (most common), BR, PL, FCR.
The presence of an oblique pulley of the thumb is essential
to FPL function.
79. When pulleys need to be reconstructed, Excessive scarring bed & Joint
Instabilities - secondary reconstruction of the FPL tendon - prefer to
reconstruct the pulleys over a silicone rod at a first stage and reconstruct
the flexor tendon later.
Aim at - 30-40 degrees of IP joint motion postop - to have fine pinch
function Good Result
Pulvertaft’s policy - allowing a minimum of 6 months between injury and
reconstruction and between the stages of a two-stage procedure –
recommended.
80.
81. Tenolysi
s -
On Examination - wide discrepancy between active and passive range of digital
motion,
Flexor tenolysis is indicated - digital flexion is reduced due adhesions in a bed of
scar tissue - restricts tendon gliding & active ROM,
Before planning - the patient should be well motivated for prolonged rehabilitation.
Goal - Independent and wide active motion of FDS & FDP – after surgery.
Oral ibuprofen administration limited adhesion formation after FDP repair.
Tenolysis is attempted –
1. After an interval of 3–6 months of primary tendon repair / tendon grafting.
2. After good fracture healing
85. Chronic mallet injuries with or without Swan
neck deformity
Doyle - > 4 weeks
Splint / Direct tendon repair / Skin imbrications (or both).
> 6 months
Tendon rebalancing with a central slip tenotomy (Fowler tenotomy),
SORL reconstruction using a lateral band or tendon graft.
Arthrodesis is a salvage procedure - Arthritic changes.
Tendon grafting - Tendon-bone construct harvested from the ECRB–
third metacarpal junction.
103. Chronic Zone 6 injuries
Side-to-side transfer
Tendon grafts – TFL / PL / Plantaris etc
In severe tendon loss - a two-stage reconstruction with silicone
rods (in literature)
Composite Vascularized tissue transfers – Dorsalis pedis
cutaneotendinous free flap / Radial artery or ulnar artery based
island flap with vascularized tendon,