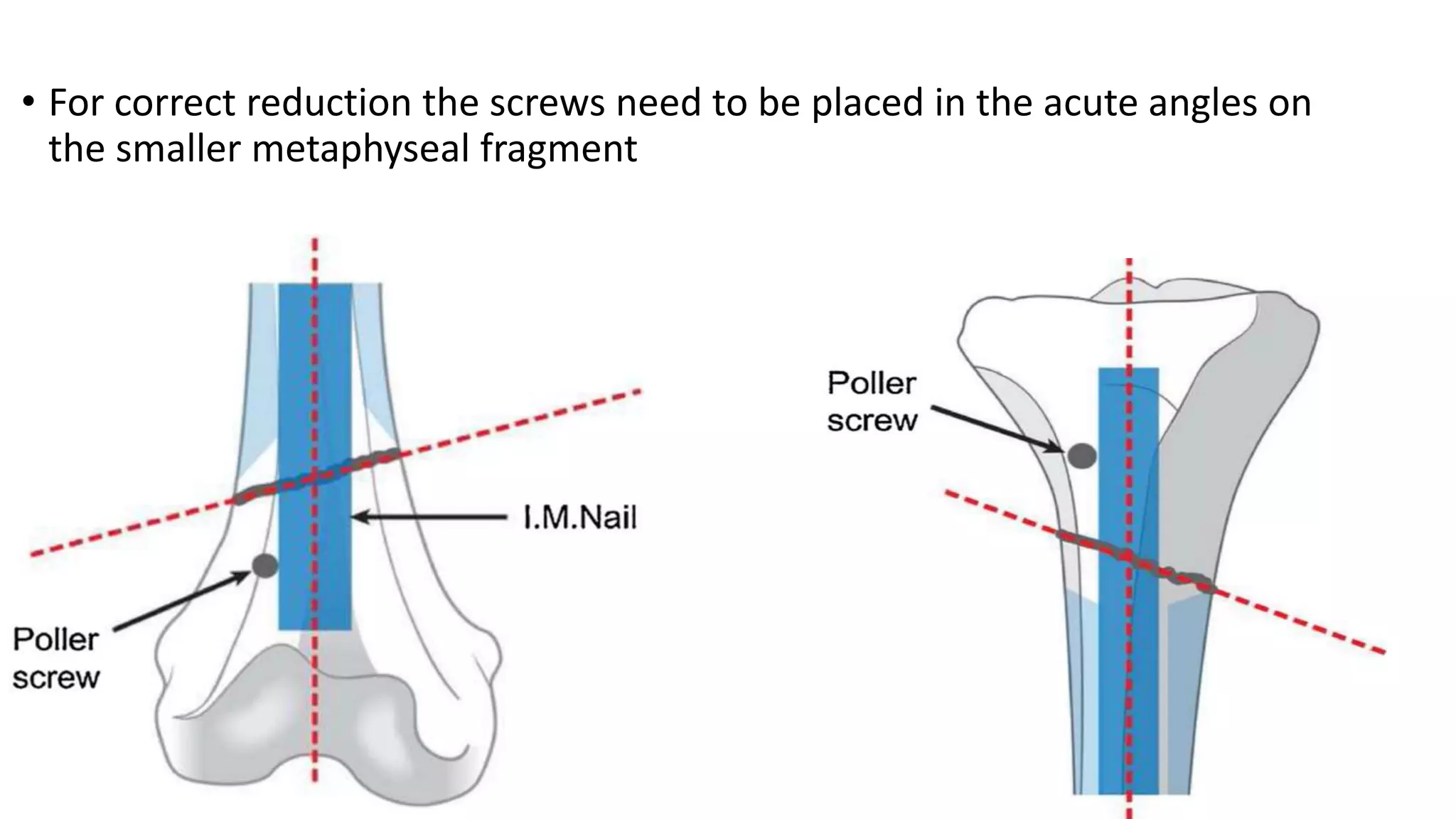
Poller screws, also known as blocking screws, are non-interlocking screws placed outside an intramedullary nail to improve fracture reduction and fixation. They provide a more rigid construct by serving as a surrogate cortex where nail-cortex contact is insufficient. Their placement helps centralize the guidewire in the medullary canal and maintains reduction through a blocking effect. While there is no consensus on their exact placement, they are generally inserted on the concave side of expected deformities to prevent malalignment during nailing.