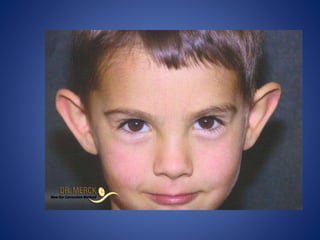
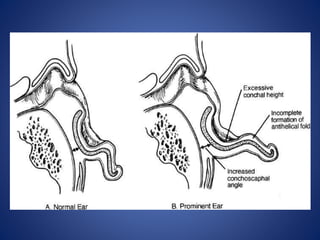
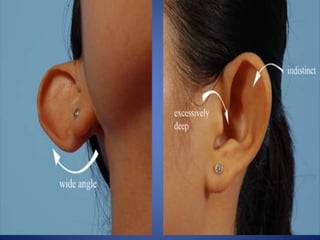
1) Prominent ears, also called protruding ears, refer to ears that stick out more than 2cm from the head or form an angle greater than 25 degrees. 2) The three main anatomic causes are underdeveloped antihelical fold, prominent concha, and protruding earlobe. 3) The goals of otoplasty are for the helical rim to be visible from the front and straight from the back with natural contours from the side.