Downloaded 85 times
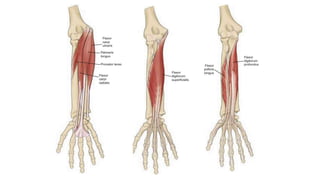
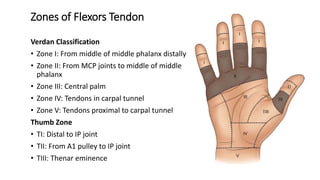
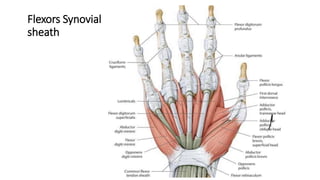
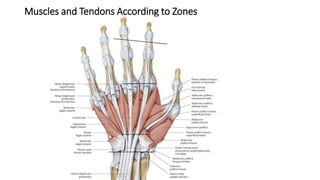
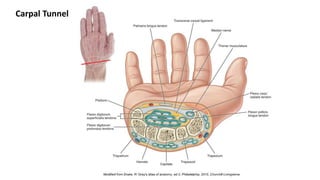
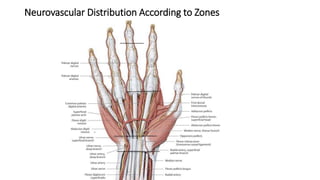
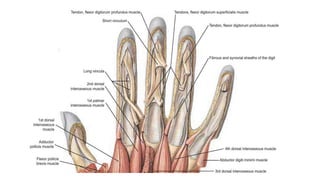

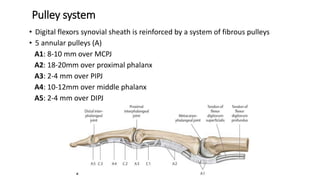
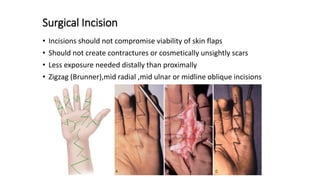

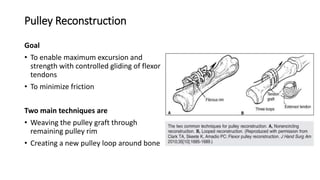

The document discusses flexor tendon injuries, including anatomy, classification by zones, surgical techniques for repair, and postoperative rehabilitation. It covers the superficial and deep flexor tendon groups, pulley system anatomy and its importance, and surgical approaches and repair methods for injuries in different zones of the hand. Primary goals of repair include restoring tendon continuity and gliding while preventing adhesions through techniques like circumferential suturing.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







