Downloaded 1,315 times
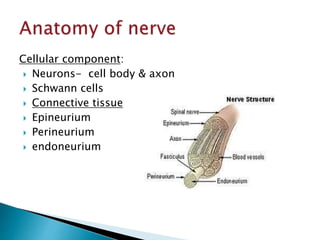
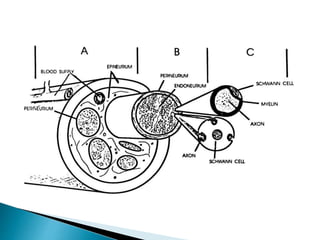

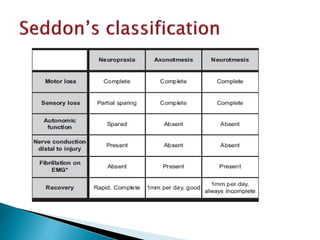
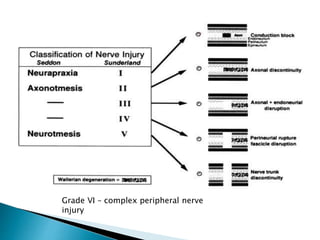
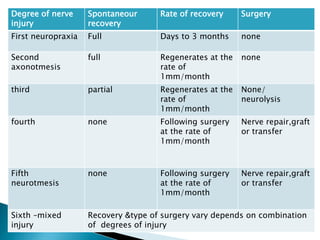

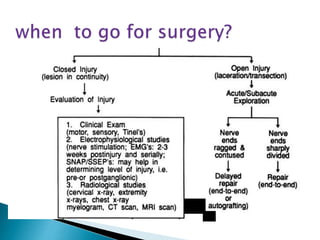
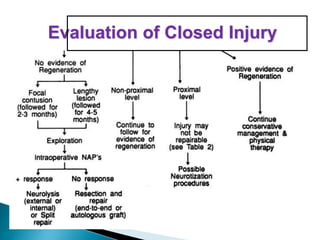
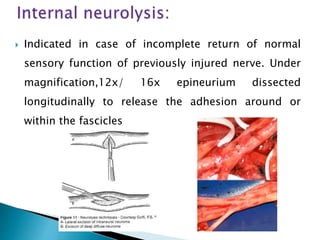
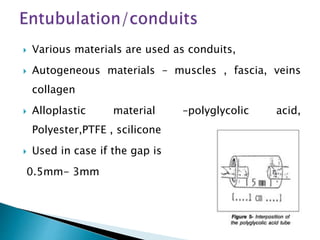

This document discusses the anatomy and classification of peripheral nerve injuries. It begins by describing the cellular components of nerves, types of nerve fibers, and classifications of nerve injuries including Seddon's and Sunderland's. It then discusses signs and symptoms of nerve injuries, common sites of injury, Wallerian degeneration, nerve regeneration, and various surgical and non-surgical treatment options including neurolysis, nerve grafting, and nerve repair. Classification of injuries is based on damage to nerve components and ability for spontaneous recovery. Surgical treatment depends on the degree and severity of injury.











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)