Downloaded 106 times
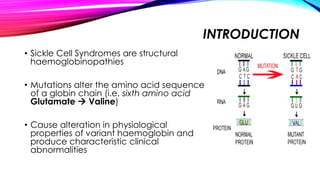
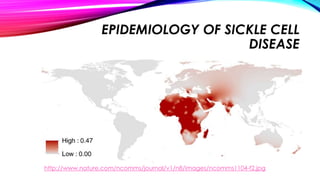
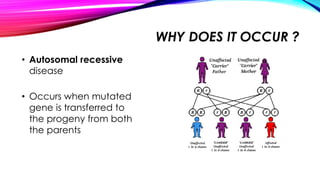
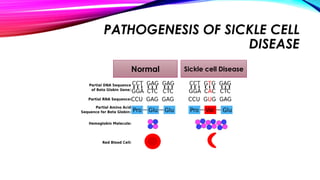
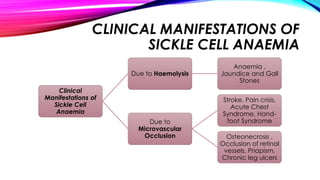
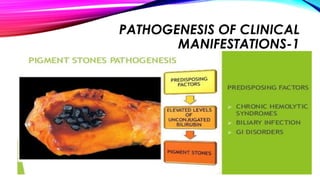
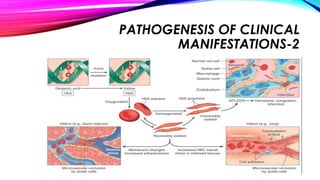
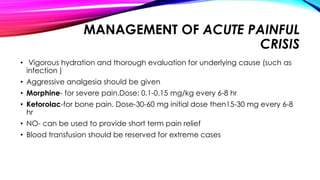


This document discusses sickle cell syndromes, which are structural hemoglobinopathies caused by mutations that alter the amino acid sequence of a globin chain. There are several types of sickle cell syndromes, including sickle cell trait, sickle cell anemia, and combinations with thalassemia. Sickle cell disease occurs due to an autosomal recessive gene being inherited from both parents. Clinical manifestations include anemia, jaundice, gallstones, pain crises, acute chest syndrome, and organ damage, due to hemolysis and microvascular occlusion of red blood cells that have sickled. Management involves treatment of acute painful crises and chest syndrome with hydration, analgesics, oxygen, and blood transf






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






