Downloaded 651 times



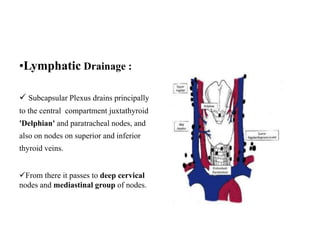





































The document provides an overview of the surgical anatomy, development, blood supply, lymphatic drainage, and examination of the thyroid gland. It discusses the thyroid gland's location in the lower neck, its lobes and isthmus, and that each lobule contains follicles. It also reviews aspects of examining a patient such as gathering demographic details, symptoms, and performing physical exams including inspection, palpation, percussion, and auscultation of the thyroid. Common investigations and treatments are also summarized.































































![Dr.Ashish Mishra Seminar Thyroid disorders [Autosaved].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/dr-230822194745-383295a9-thumbnail.jpg?width=640&height=640&fit=bounds)































