Approach to Patient with Pallor: Causes, Evaluation, and Management
•Download as PPT, PDF•
24 likes•9,106 views

This document discusses the approach to evaluating a patient presenting with pallor. It begins by outlining the learning objectives which are to understand the importance of history and exam in workup of pallor, learn about causes and classification of anemia, how to interpret lab tests, and management of anemia. It then provides details on evaluating pallor, the definition of anemia, essential initial lab tests, and an approach to diagnostic workup of anemia based on mean corpuscular volume. Case examples are presented and discussed to demonstrate examples of iron deficiency anemia, vitamin B12/folate deficiency anemia, and sickle cell anemia. Management of iron deficiency anemia is also reviewed.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Approach to Patient with Pallor: Causes, Evaluation, and Management
Similar to Approach to Patient with Pallor: Causes, Evaluation, and Management (20)
More from DOCTOR WHO
More from DOCTOR WHO (20)
Recently uploaded
Recently uploaded (20)
Approach to Patient with Pallor: Causes, Evaluation, and Management
- 1. Approach to patient with Pallor
- 2. Learning objectives 1. To understand the importance of proper history and clinical examination in the workup of a patient presenting with pallor in various age groups. 2. Causes and classification of Anemia 3. Interpretation of Lab. Investigations for diagnostic purposes. 4. understanding of ordering specific investigations for confirmation and finding out the cause of Anemia. 5. To describe the management plan of anemia in various conditions and to ensure proper replacement therapy.
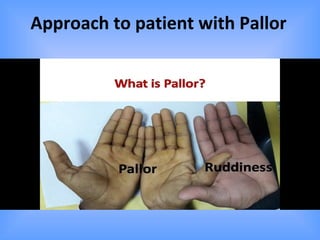
- 3. Pallor • Pale color of the skin and mucous membrane due to deficiency of hemoglobin. (hemoglobin in carried in the RBCs) There are many causes of pallor : Anemia : Most common Heart disease Sleep deprivation Shock : septic , Anaphylactic, Cardiogenic, Neurogenic or hypovolemic
- 4. Pallor is also seen in case of Endocrine defect : 1.long standing diabetes leading to keratin deposition in the skin 2. Hypothyroidism with or without anemia 3.Hypopituitarism leading to decrease in the melanin stimulatory hormone Pallor is seen in : * Palm creases * Conjunctiva. * And mucous membranes
- 5. Pallor in mucus membrane of lower eye lid and conjunctive
- 6. Angular cheilitis (AC) is inflammation of one or both corners of the mouth.
- 7. Angular chelosis & Glossitis
- 8. Koilonychia in Iron def.
- 9. Iron Deficiency Anemia - koilonychia
- 10. Case Presentation • HISTORY: A 60- year- old male presented with marked pallor, easy fatigability and breathlessness on exertion. On questioning he revealed that he is taking pain killers for his joint pains for the last 3 years. He mentioned about passing dark colored stools off and on. • On examination, he was markedly pale, tachycardia and having spoon shaped deformity of nails. • Blood examination: Hemoglobin 7 g/dl • MCV: 68 fl, MCHC: • Raised Iron binding capacity with serum Ferritin 12ug/l (Normal range 60 or above ug/l)
- 12. Anemia is defined by • Reduction in Hg Concentration, •Hct Concentration or • RBC count according to the age & sex of the individual
- 13. 13 Considerations by Age, Sex, and Other Factors 1 of 2 • Newborns less than one week old have hemoglobin of 14-22 g/dl. • By six months , hemoglobin levels are11 and 14 g/dl. • 1 year and 15 years hemoglobin is 11-15 g/dl. • Normal adult hemoglobin depends on gender: – ♀ 12-16 g/dl – ♂ 14-18 g/dl • In geriatric age group, men and women have same hemoglobin range: 12-16 g/dl.
- 14. Symptoms • Exertional dyspnea and Dyspnea at Exertion • Headaches • Fatigue • Bounding pulses and Roaring in the Ears • Palpitations • PICA is an eating disorder typically defined as the persistent ingestion of nonnutritive substances for at least 1 month at an age for which this behavior is developmentally inappropriate.
- 15. Etiology of anemia • Iron deficiency 25% • Anemia of inflammation 25% • Hemoglobinopathy 25% • Hemolytic anemia/marrow failure 15% • Myelodysplasia 10%
- 16. First Step in Evaluation Clinical PresentationClinical Presentation
- 17. 17 Approach • Detailed History • Review of Systems • Physical Exam • Laboratory Evaluation – Prior documentation of CBC’s – CBC with RETICULOCYTE COUNT – Review peripheral blood smear
- 18. 18 History Family historyFamily history Spherocytosis Sickle cell anemia Thalassemia DietDiet Vegetarian Drugs/Toxins Infection Alcohol AbuseAlcohol Abuse Folate deficiency Liver disease MalabsorptionMalabsorption B12 Folate Iron Exposure Lead Chemotherapy Peptic UlcerPeptic Ulcer DiseaseDisease DiverticulitisDiverticulitis Colonic PolypsColonic Polyps GI MalignancyGI Malignancy colorectal esophageal Recent SurgeryRecent Surgery TravelTravel
- 19. Symptoms Weakness Fatigue Dizziness Headache Chest pain SOB / DOE Palpitations Cold intolerance Dysphagia Jaundice Hematemesis Diarrhea Constipation Melena Hematuria Menorrhagia Pica (clay, dirt, chalk, ice) Hematoma
- 20. Physical Exam
- 21. 21 Physical Exam Ophtho exam Flame hemorrhage Papilledema Exudates Pallor Blue sclera Angular Cheilitis Iron Deficiency GlossitisGlossitis B12 / Folate / Iron Tachycardia Jaundice Liver Disease Hemolysis Guiaic positive (gFOBT) Splenomegaly Malignancy Infection Liver disease Chronic Hemolysis Adenopathy SkinSkin Pallor Ulcerations Scars Thin/Brittle, Spoon- shaped nails Edema Neurologic Headache, fatigue Lack of concentration Syncope Paresthesias Ataxia Dementia
- 22. Essential laboratory tests in the evaluation of anemia • Hemoglobin – amount of lysed pigment in a volume of blood • Mean corpuscular volume – size of red blood cells • Red cell distribution width – measure of variation of cell size • Red blood cell count – absolute number of red blood cells per volume • Platelet count • White blood cell count • Peripheral blood smear
- 23. Diagnostic approach to anemia 1. Review prior CBCs 2. Take comprehensive history and physical 3. Classify anemia by MCV – Microcytic (MCV <80 fL) – Normocytic (MCV 80-100 fL) – Macrocytic (MCV >100 fL) • Mild macrocytosis MCV 100-110 fL • Marked macrocytosis MCV >110 fL 1. Reticulocyte Count (classification of proliferation) 2. Order appropriate additional tests
- 24. Case 1 • 52 year old male construction worker with presenting complaint of fatigue for 2 months. He now reports getting dyspnea when climbing stairs or carrying heavy loads at work. He says, “I never go to doctors.” • Physical exam unremarkable • ROS occasional crampy abdominal pain
- 25. Case 1 • Hgb 10.2 gm/dl, MCV 68 fL, Platelets 450,000/dL • How do you classify the anemia?
- 26. Case 1 • Serum Iron is low • Fecal occult blood test is positive Copyright ©2002 American Society of Hematology. Copyright restrictions may apply.
- 27. Features of iron deficiency anemia • Clinical – Symptoms of anemia – Evidence of blood loss – Pica (very specific) • Laboratory – Microcytic anemia (occasionally normocytic) – Elevated RDW – Elevated platelet count – Low serum iron, ferritin and elevated TIBC
- 29. 29 Iron Deficiency – Etiologies • History –History – GI (blood loss, diarrhea/constipation),GI (blood loss, diarrhea/constipation), menses, coagulopathy, urine color (menses, coagulopathy, urine color (cokecoke-colored-colored [bilirubin] OR[bilirubin] OR redred [hematuria, hemoglobinuria])[hematuria, hemoglobinuria]) • Guaiac stoolsGuaiac stools – Office DRE – Hemocult cards as outpatient • Colonoscopy / EGDColonoscopy / EGD • PT / APTT, UAPT / APTT, UA
- 30. Case 2 • 48-year-old white man is referred for pallor and unexplained tierdness. He is an executive in a software company and reports fatigue and dyspnea during brisk walk • Physical examination: He is a normal, healthy-looking man, perhaps pale, with a clean tongue. The results of his chest, abdomen, and neurologic exams are all normal.
- 31. Case 2 • Hemoglobin 9.2 gm/dl • Mean corpuscular volume (MCV) 112 fL • White blood cells 3,400/ul normal differential • Platelets 89,000/ul
- 32. Case 2 laboratory results • B12 level 100 pg/mL, folate >20 ng/mL Copyright ©2001 American Society of Hematology. Copyright restrictions may apply. Schrier, S. ASH Image Bank 2001;2001:100231
- 33. Case 3 • 45 year old African-American female presents with fatigue for 6 months. She now only works 6 hours a day at her secretarial job and is now dyspneic climbing 2 flights of stairs at home. • PMH: Hypertension, depression, G6P6 • PSH: C-section x 2, breast biopsy – benign • FH: Father – multiple myeloma, Mother – DM2 on hemodialysis, 2 younger siblings are well • SH: No tobacco or alcohol • ROS: Joint pains for about 6 months, intermittent chest pain worse with deep breathing • Medications: Lisinopril, aspirin, venlafaxine
- 34. Case 3 • Hemoglobin 8.0 gm/dL • MCV 81 fL • WBC 3,200/uL • Platelets 450,000/uL
- 35. Management of iron deficiency • Rule out blood loss, reason for negative iron balance – Gastrointestinal – Genitourinary – Poor iron absorption – Pregnancy
- 36. Oral iron supplementation • Goal: 150-200 mg elemental iron daily • Administration – DO NOT give with food – Give 2 hrs from antacids – May give with ascorbic acid 250 mg • Gastrointestinal intolerance (~20%) – Decrease daily elemental iron dose • Switch from sulfate to gluconate or elixir – Give with food (will decrease absorption)
- 37. Reticulocytes
- 38. Interpreting reticulocyte counts • Reticulocytes are erythrocytes new to peripheral circulation • Need to correct for degree of anemia – Reticulocyte index = Retic % x [Pt Hct/NlHct] – Absolute reticulocyte count = Retic % x RBC number • Appropriate reticulocytosis – Reticulocyte index >2% – Absolute reticuocyte count >100,000/mcl
- 39. Anemia in the elderly 10-30% of elderly are anemic • Consequences – Decreased physical performance – Increased mortality in CHF patients – EPO improved LV function in elderly CKD patients treated with EPO • About 30% have “unexplained anemia” Guralnik J Hematology: ASH Education Book 2005
Editor's Notes
- Hemoglobin is a MEASURED value, and thus is more reproducible in contrast to the hematocrit which is caluclated a subject to other variations such as plasma volume.