1. The study examined gene frequencies and disease characteristics of sickle cell disease among tribal and Chetti communities in Wayanad district, Kerala, India.
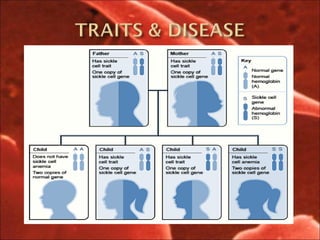
2. Gene frequencies for the sickle cell trait ranged from 1.9-19.6% across communities, with the highest in Wayanadan Chettis. Many homozygotes were observed with the oldest being 48 years old.
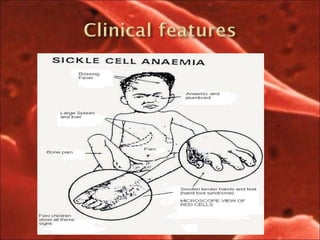
3. The disease was mild in 52.2% of cases, with painful crises in 43.5% and splenomegaly and leg ulcers each in 4.3%. Survival of patients appears higher in Kerala than other states.