Downloaded 119 times
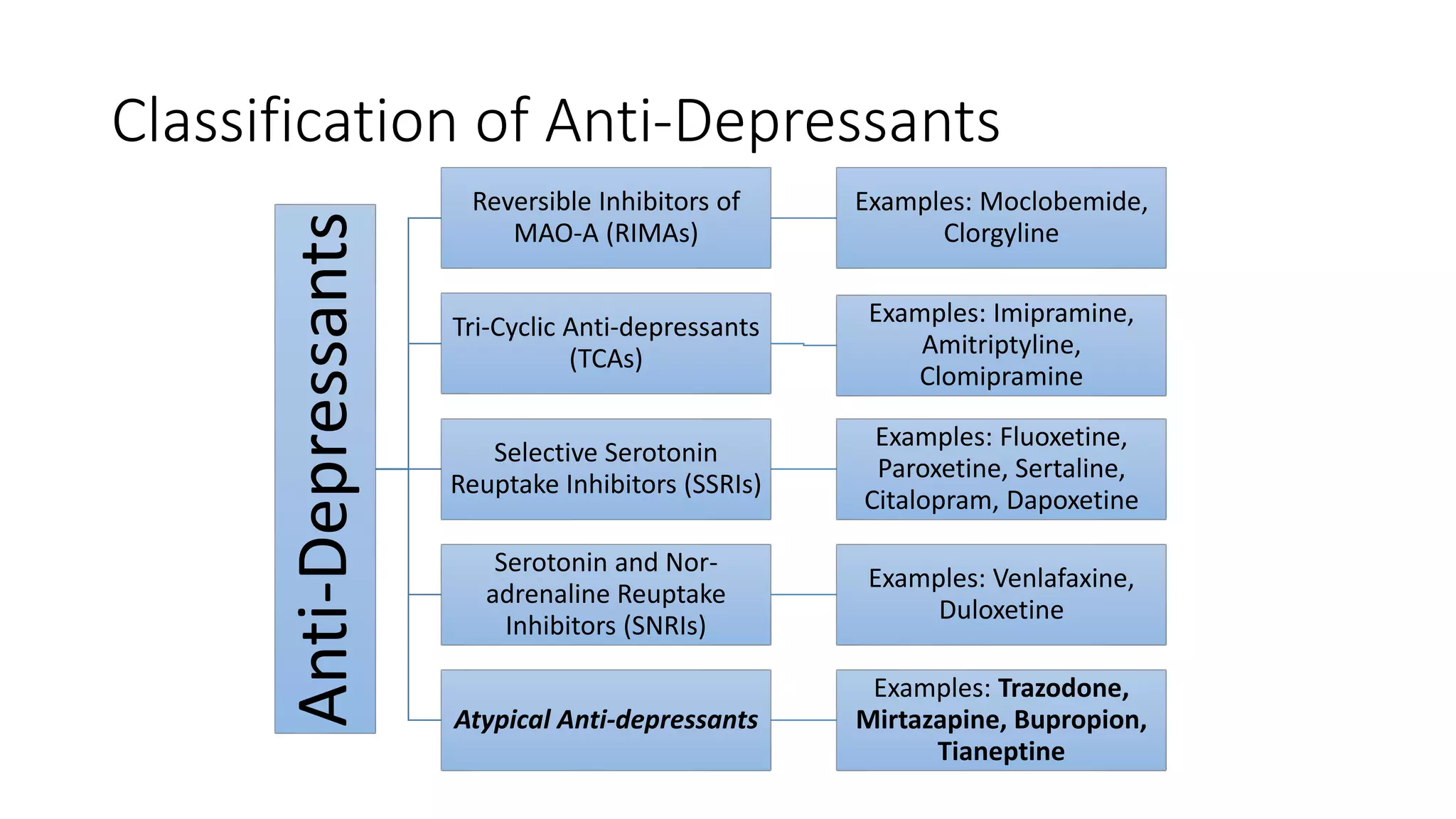
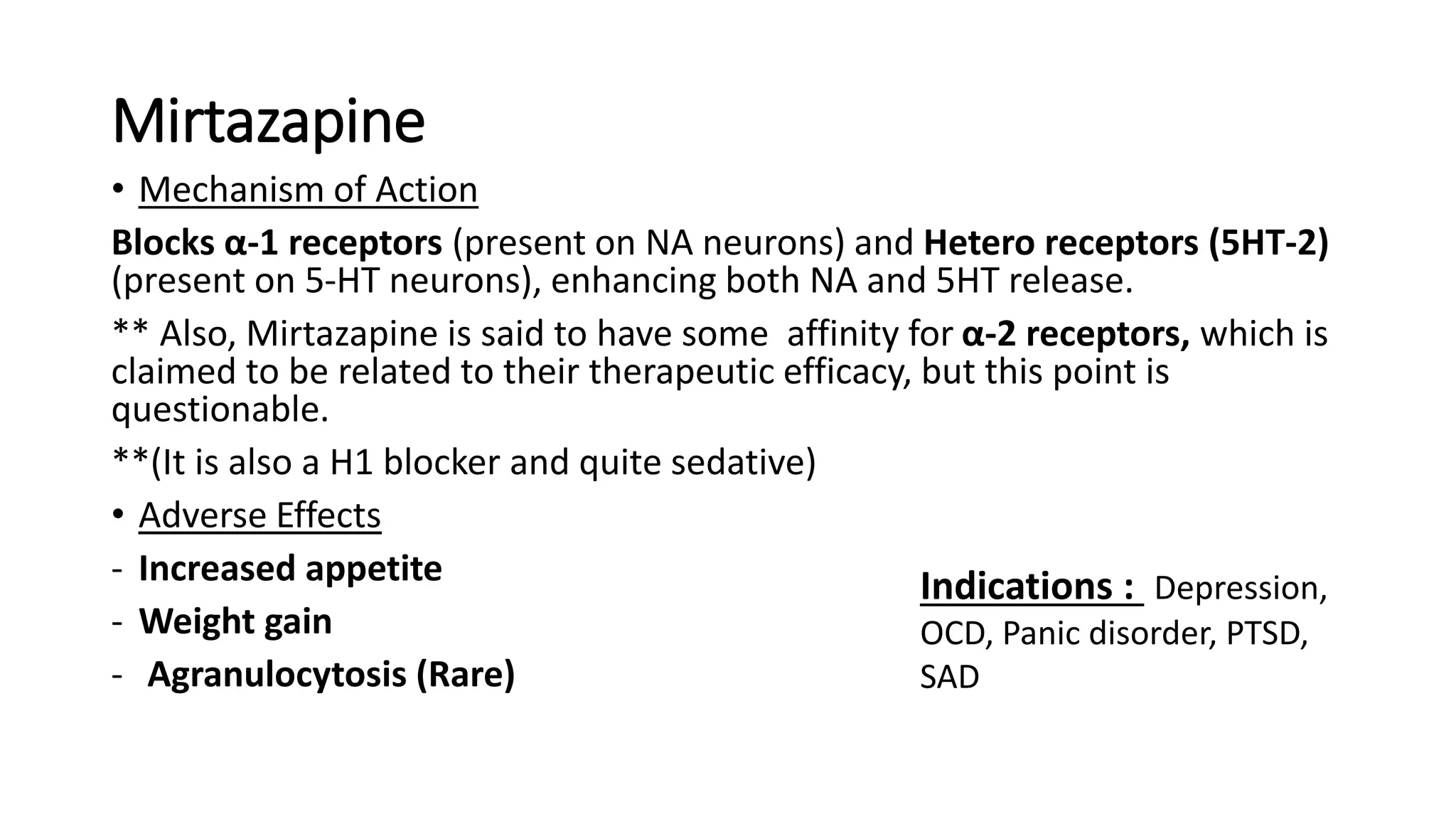
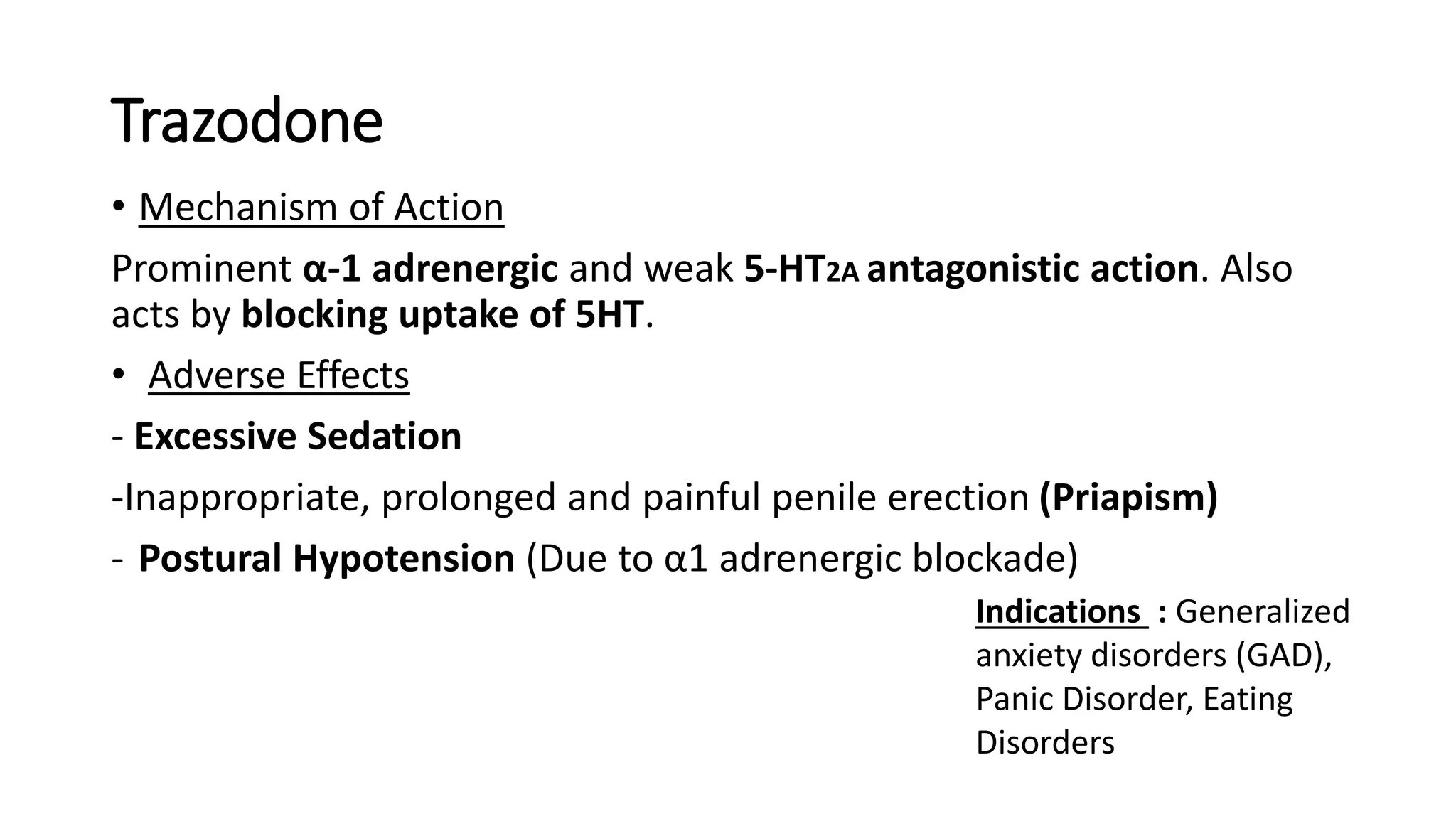




The document reviews atypical antidepressants, detailing their classification, mechanisms of action, indications, and side effects. It covers various types of antidepressants, including monoamine oxidase inhibitors, tricyclics, SSRIs, SNRIs, and specific atypical agents like mirtazapine, trazodone, and bupropion. The document also discusses the pathophysiology of depression, emphasizing the role of neurotransmitter imbalances.
































































































