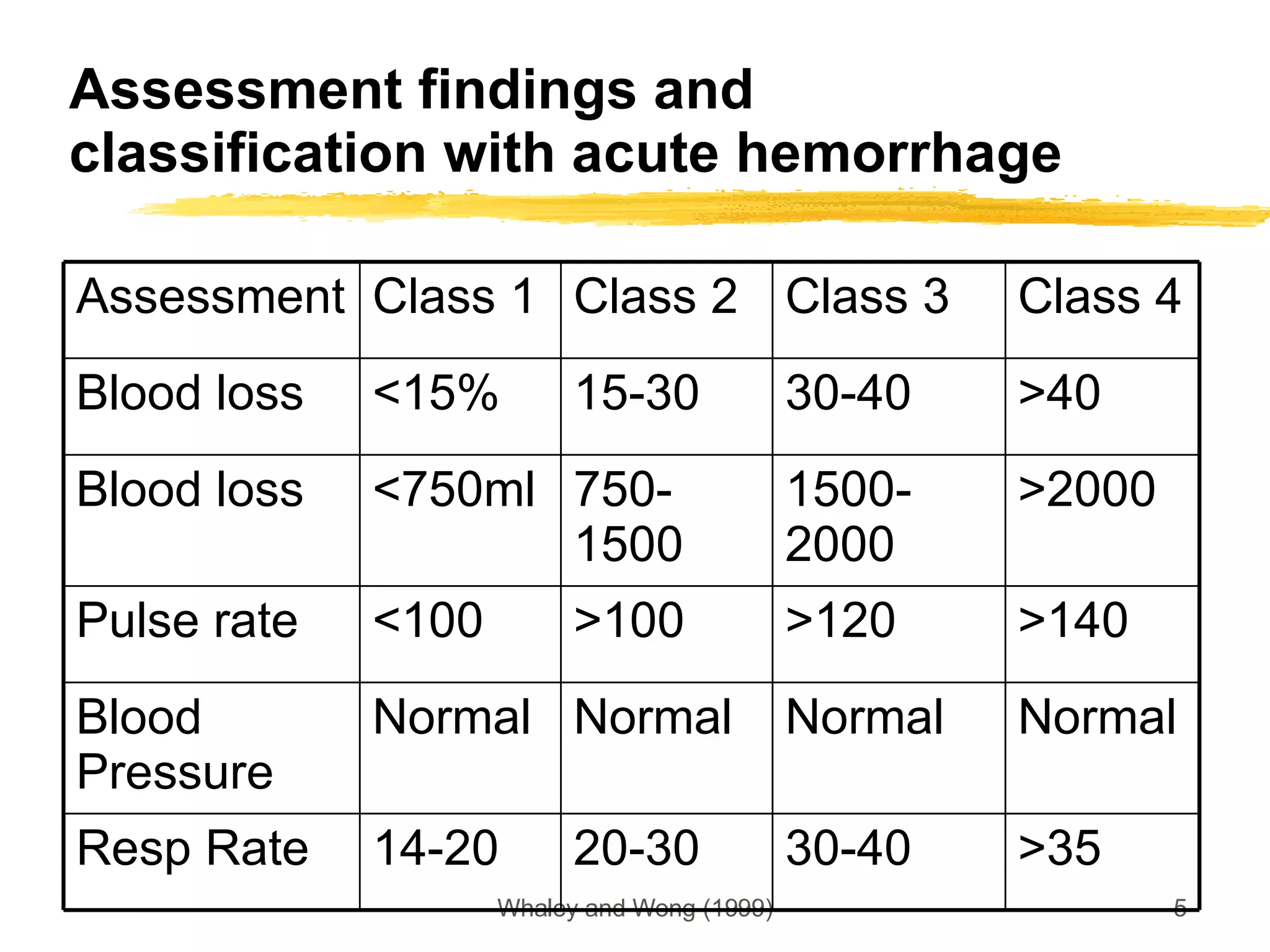
This document discusses the identification and treatment of various types of shock states. It defines hypovolemic, distributive, cardiogenic, and septic shock and their clinical manifestations. Early diagnosis is key, involving history, physical exam assessing vital signs, perfusion, and urinary output. Treatment focuses on establishing airway, supplying oxygen, restoring circulating volume with fluids, and using vasopressors to improve cardiac output as needed based on the type and severity of shock. Children in particular can maintain blood pressure while showing signs of poor peripheral perfusion.











































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









