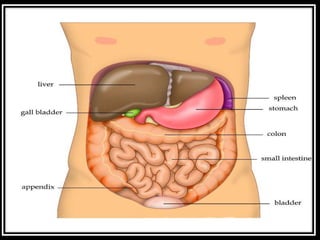
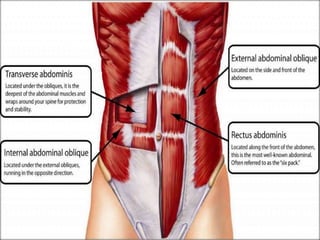
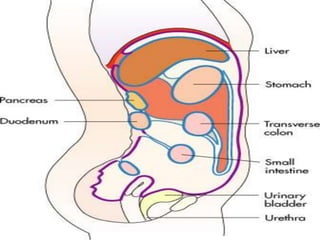
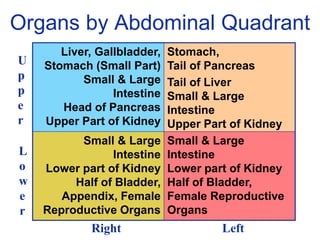
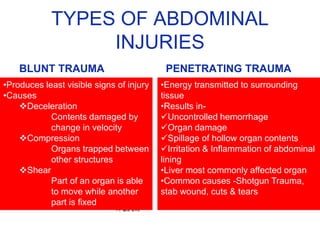
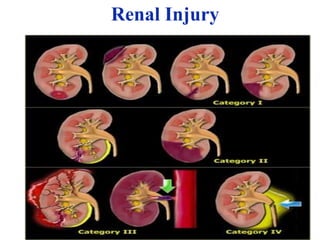
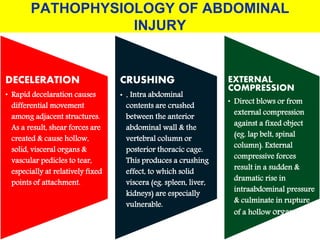
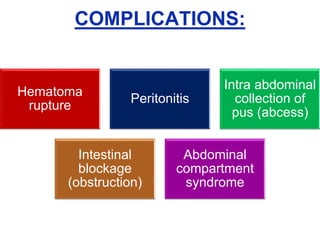
The document provides a comprehensive overview of abdominal injuries, including their anatomy, types, clinical manifestations, and management strategies. It discusses injuries to various organs such as the diaphragm, liver, spleen, and intestines, detailing symptomatology and treatment protocols based on the severity of the injury. Additionally, it emphasizes diagnostic studies, complications, and nursing management pertaining to abdominal trauma.