Downloaded 3,915 times


![• Arterio-Venous ECMO (AV ECMO) :
An arteriovenous (AV) extracorporeal circuit that uses the
patient’s own arterial pressure or incorporates a pump to drive
blood across an oxygenator can partially support the
respiratory system by effectively removing carbon dioxide
(CO2) (extracorporeal CO2 removal [ECCO2R]).
ECMO guidelines AlfredHealth Update nov 2015](https://image.slidesharecdn.com/ecmofinal-160719115713/85/ECMO-extracorporeal-membrane-oxygenation-26-320.jpg)
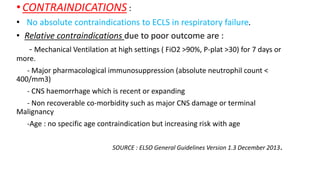
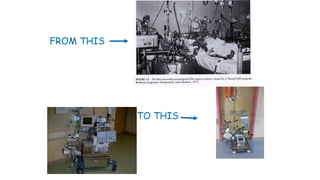
![Chest X-ray belongs to a 19-yr-old female with ARDS on VV-ECMO.
Guillermo Martinez, and Alain Vuylsteke Contin Educ
Anaesth Crit Care Pain 2011;bjaceaccp.mkr056
© The Author [2011]. Published by Oxford University Press on behalf of the British Journal of
Anaesthesia. All rights reserved. For Permissions, please email:
journals.permissions@oup.com](https://image.slidesharecdn.com/ecmofinal-160719115713/85/ECMO-extracorporeal-membrane-oxygenation-66-320.jpg)





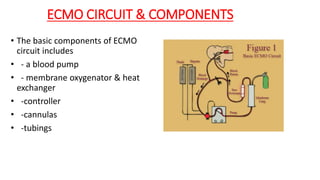
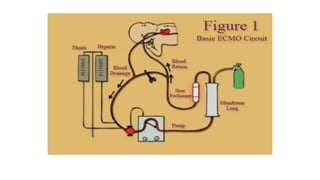
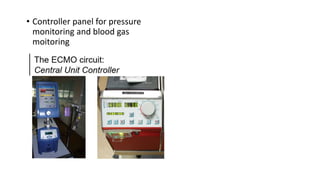
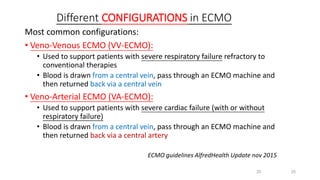
This document provides an overview of extracorporeal membrane oxygenation (ECMO), including its history, principles, components, indications, and complications. Some key points: - ECMO is a form of extracorporeal life support that oxygenates blood and removes carbon dioxide outside of the body, then returns the blood to the patient. It has been used since the 1950s and is now standard treatment for some cardiac and respiratory conditions. - The basic ECMO circuit includes a blood pump, membrane oxygenator, heat exchanger, cannulas, and tubing. There are various configurations depending on whether it is used for respiratory (VV ECMO) or cardiac (VA ECMO) support. -