Downloaded 130 times

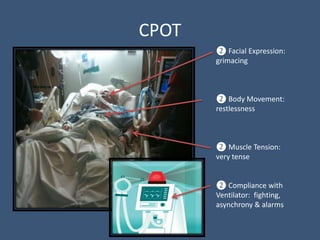
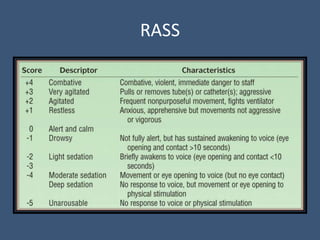
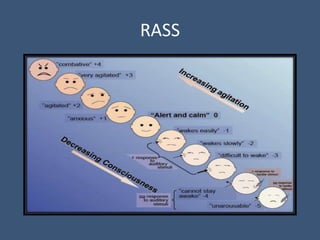


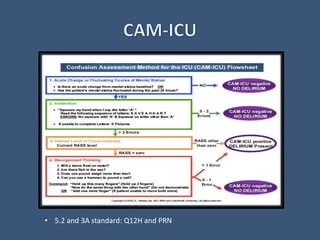



The document discusses tools for assessing pain, agitation, and delirium in ICU patients: CPOT for pain, RASS for sedation level, and CAM-ICU for delirium. CPOT, RASS, and CAM-ICU are simple, non-invasive tools that can improve patient outcomes by focusing nursing interventions. The document provides details on how to use each tool, including how often they should be administered. It also discusses the importance of detecting and managing delirium in ICU patients.















































































