Shock – ASurgical Perspective
Moderator Dr Arun Rathore
Dr Bhavana Verma
Presentor Dr Vishal Verma
2.
Introduction
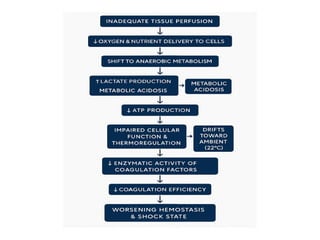
• Shock isa life-threatening condition due to
inadequate tissue perfusion and oxygenation.
• It leads to cellular hypoxia, organ dysfunction,
and, if untreated, death.
• Early recognition and management are key to
improving survival outcomes.
• Shock occursat 3 anatomical areas of CVS
1. Heart/Cardiogenic
– Extrinsic- tension pneumothorax, hemothorax, cardiac
tamponade
– Intrinsic-MI, cardiac contusion, cardiac failure
2. Large and medium vessels/Hemorrhagic
– Blood loss
3. Small vessels/Distributive
– Neurological dysfunction or sepsis leads to
vasodialtation
5.
Hypovolemic Shock
Definition: Causedby a decrease in intravascular
volume, leading to decreased cardiac output and
hypoperfusion.
Causes:
- Hemorrhage: Trauma, GI bleeding, ruptured
aortic aneurysm.
- Non-hemorrhagic: Burns, severe dehydration
(vomiting, diarrhea), third-spacing (pancreatitis,
peritonitis).
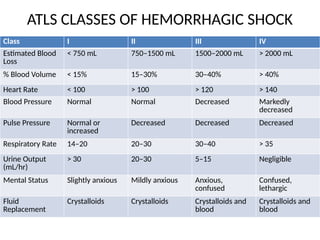
ATLS CLASSES OFHEMORRHAGIC SHOCK
Class I II III IV
Estimated Blood
Loss
< 750 mL 750–1500 mL 1500–2000 mL > 2000 mL
% Blood Volume < 15% 15–30% 30–40% > 40%
Heart Rate < 100 > 100 > 120 > 140
Blood Pressure Normal Normal Decreased Markedly
decreased
Pulse Pressure Normal or
increased
Decreased Decreased Decreased
Respiratory Rate 14–20 20–30 30–40 > 35
Urine Output
(mL/hr)
> 30 20–30 5–15 Negligible
Mental Status Slightly anxious Mildly anxious Anxious,
confused
Confused,
lethargic
Fluid
Replacement
Crystalloids Crystalloids Crystalloids and
blood
Crystalloids and
blood
8.
Clinical Features:
• Tachycardia-highlyunreliable
• hypotension, weak pulses.
• Cold and clammy skin-stagnation of venous
blood and rapid cessation of arterialization of
of blood.
• Oliguria
• altered mental status.
9.
COMPENSATORY MECHANISM
Hormonal Response:
•Angiotensin II increases sympathetic activity, releasing
hormones (epinephrine, norepinephrine, dopamine) from
the adrenal medulla. These help maintain vascular volume
and blood pressure.
• Cortisol and aldosterone from the adrenal cortex promote
fluid equilibrium, sodium recovery, and water retention to
support blood volume.
• ADH (Antidiuretic Hormone): Released from the pituitary
to retain water in the kidneys, helping maintain
intravascular volume during shock.
Management:
- **Oxygen andventilation support** (consider
intubation if severe).
- **Pharmacological support**: Inotropes
(Dobutamine, Milrinone), Vasopressors
(Norepinephrine).
- **Revascularization**: PCI or CABG if AMI-
related.
- **Diuretics** for pulmonary congestion.
15.
Septic Shock
Definition: Atype of distributive shock caused
by systemic infection and inflammatory
response.
Causes:
- Pneumonia, urosepsis, intra-abdominal
infections.
- Skin/soft tissue infections (necrotizing fasciitis).
- Immunosuppression increases susceptibility.
16.
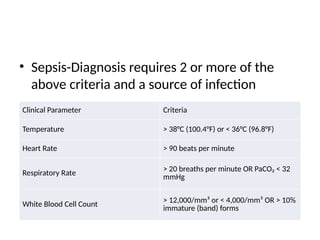
• Sepsis-Diagnosis requires2 or more of the
above criteria and a source of infection
Clinical Parameter Criteria
Temperature > 38°C (100.4°F) or < 36°C (96.8°F)
Heart Rate > 90 beats per minute
Respiratory Rate > 20 breaths per minute OR PaCO₂ < 32
mmHg
White Blood Cell Count > 12,000/mm³ or < 4,000/mm³ OR > 10%
immature (band) forms
17.
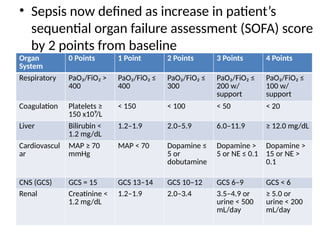
• Sepsis nowdefined as increase in patient’s
sequential organ failure assessment (SOFA) score
by 2 points from baseline
Organ
System
0 Points 1 Point 2 Points 3 Points 4 Points
Respiratory PaO₂/FiO₂ >
400
PaO₂/FiO₂ ≤
400
PaO₂/FiO₂ ≤
300
PaO₂/FiO₂ ≤
200 w/
support
PaO₂/FiO₂ ≤
100 w/
support
Coagulation Platelets ≥
150 x10⁹/L
< 150 < 100 < 50 < 20
Liver Bilirubin <
1.2 mg/dL
1.2–1.9 2.0–5.9 6.0–11.9 ≥ 12.0 mg/dL
Cardiovascul
ar
MAP ≥ 70
mmHg
MAP < 70 Dopamine ≤
5 or
dobutamine
Dopamine >
5 or NE ≤ 0.1
Dopamine >
15 or NE >
0.1
CNS (GCS) GCS = 15 GCS 13–14 GCS 10–12 GCS 6–9 GCS < 6
Renal Creatinine <
1.2 mg/dL
1.2–1.9 2.0–3.4 3.5–4.9 or
urine < 500
mL/day
≥ 5.0 or
urine < 200
mL/day
18.
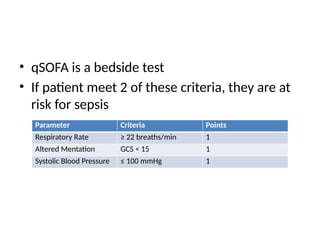
• qSOFA isa bedside test
• If patient meet 2 of these criteria, they are at
risk for sepsis
Parameter Criteria Points
Respiratory Rate ≥ 22 breaths/min 1
Altered Mentation GCS < 15 1
Systolic Blood Pressure ≤ 100 mmHg 1
Management:
- **IV Fluids**:30 mL/kg crystalloid bolus.
- **Vasopressors**: Norepinephrine if
hypotension persists.
- **Broad-spectrum IV antibiotics within 1
hour.**
- **Source control**: Drain abscess, remove
infected devices.
22.
Neurogenic Shock
Definition: Causedby loss of sympathetic tone
following spinal cord injury or trauma.
Causes:
- High spinal cord injury (Cervical, upper
thoracic).
- Traumatic brain injury (TBI).
- Epidural or spinal anesthesia complications.
Management:
- **IV Fluidsfirst-line** to restore intravascular
volume.
- **Vasopressors** (Norepinephrine, Dopamine)
for BP support.
- **Atropine** for severe bradycardia.
- **Spinal immobilization and high-dose steroids
if indicated.**
26.
Obstructive Shock
Definition: Dueto mechanical obstruction of blood
flow, leading to inadequate cardiac output.
Causes:
- **Tension Pneumothorax**: Air trapping
compresses heart/lungs.
- **Cardiac Tamponade**: Pericardial fluid restricts
heart filling.
- **Massive Pulmonary Embolism (PE)**: Clot
blocks pulmonary circulation.
![How to manage lethal triad
• Acidosis- correct underlying cause
– Blood product
– Fluids
– NaHCO3
– THAM- Tromethamine; tris[hydroxymethyl] aminomethane- inert amino
alcohol that buffer CO2 and acids
• Hypothermia
– Passive-warmed iv fluids, blankets, warm rooms
– Active external warming- heating pad & radient warmers
– Active internal warming- Cavity lavage, warmed fluids
• Coagulopathy
– Prothrombin complex concentrate PCC>FFP
– Tranexamic acid](https://image.slidesharecdn.com/shock-250610103650-8d35841f/85/shockhemorrhadic-surgical-perspective-pptx-31-320.jpg)




































































